Branches of the superior mesenteric. Branches of the abdominal aorta. Visceral branches: middle adrenal and renal arteries
Superior mesenteric artery, a. mesenterica superior, is a large vessel that starts from the anterior superficial aorta, slightly below (1-3 cm) of the celiac trunk, behind the pancreas. Coming from under the lower edge of the gland, the superior mesenteric artery goes down and to the right. Together with the superior mesenteric vein located to the right of it, it lies on the anterior surface of the horizontal (or ascending) part of the duodenum, crosses it across, immediately to the right of the flexura duodenojejunalis. Having reached the root of the mesentery of the small intestines, the superior mesenteric artery penetrates between the leaves of the latter, forming an arch convex to the left, and reaches the right iliac fossa. Along its course, the superior mesenteric artery gives off the following branches: to the small intestine (with the exception of the upper part of the duodenum) , cecum with a vermiform appendix, ascending and partially to the transverse colon. The following arteries depart from the superior mesenteric artery.
- Inferior pancreaticoduodenal artery, a. pancreatico-duodenalis inferior (sometimes not single), originates from the right edge of the initial section of the superior mesenteric artery, goes down and to the right along the anterior surface of the pancreas, bending around its head along the border with the duodenum. The inferior pancreaticoduodenal artery gives branches to the pancreas and duodenum and anastomoses with the superior pancreaticoduodenal artery - branch of a. gastroduodenalis.
- Intestinal arteries, numbering up to 15, depart sequentially one after another from the convex part of the arch of the superior mesenteric artery. Intestinal arteries are directed between the layers of the mesentery to the loops of the jejunum and ileum - these are the jejunal arteries and ileal arteries, aa.. jejunales et aa. ilei. On its way, each branch is divided into two trunks, which anastomose with the same trunks formed from the division of adjacent intestinal arteries. Such anastomoses look like arcs or arcades. New branches extend from these arcs, which also divide, forming arcs of the second order, somewhat smaller in size. From the arches of the second order, arteries again depart, which, dividing, form arches of the third order, etc. From the last, most distal, series of arches, straight branches extend directly to the walls of the loops of the small intestines. In addition to intestinal loops, these arches give rise to small branches that supply blood to the mesenteric lymph nodes.
- Ileocolic artery, a. ileocolica, arises from the cranial half of the superior mesenteric artery, to the right of the root of the mesentery of the small intestine. Heading to the right and downward under the parietal peritoneum of the posterior abdominal wall to the end of the ileum and to the cecum, the ileocolic artery divides into two branches supplying blood to the cecum, the beginning of the colon and the terminal ileum. The branches arising from the ileocolic artery are as follows.
- Anterior and posterior cecal arteries, aa.. cecales anterior et posterior, heading to the corresponding surfaces of the cecum.
- The ileal branch is a continuation of a. ileocolica, goes down to the ileocecal angle, where, connecting with the terminal branches of aa.. ilei, it forms an arc from which branches extend to the terminal section of the ileum.
- The colon branch goes to the right towards the ascending colon. Before reaching the medial edge of this colon, it is divided into two branches, one of which, the ascending branch, g. ascendens, rises along the medial edge of the ascending colon and anastomoses (forms an arch) with a. Colica dextra; the other branch descends along the medial edge of the colon and anastomoses (forms an arch) with a. ileocolica. Branches extend from these arches, supplying blood to the ascending colon and cecum, as well as the appendix through the appendix artery, a. appendicularis.
- Right colon artery, a. colica dextra, departs from the right side of the superior mesenteric artery in its upper third, at the level of the root of the mesentery of the transverse colon, and goes almost transversely to the right, to the medial edge of the ascending colon. At some distance from the ascending colon, the right colon artery divides into ascending and descending branches. The descending branch connects to branch a. ileocolica, and the ascending branch anastomoses with the right branch of a. Colica media. From the arches formed by these anastomoses branches extend to the wall of the ascending colon, to the flexura coli dextra and to the transverse colon.
- Middle colon artery, a. colica media, departs from the initial section of the superior mesenteric artery, heading forward and to the right between the leaves of the mesentery of the transverse colon, and is divided into two branches: right and left . The right branch connects to the ascending branch a. colica dextra, and the left one, running along the mesenteric edge of the transverse colon, anastomoses with the ascending branch of a. colica sinistra, which extends from a. mesenterica inferior. Connecting in this way with the branches of neighboring arteries, the middle colon artery forms arches. From the branches of these arches, arches of the second and third order are formed, which give direct branches to the walls of the transverse colon, flexura coli dextra et sinistra.
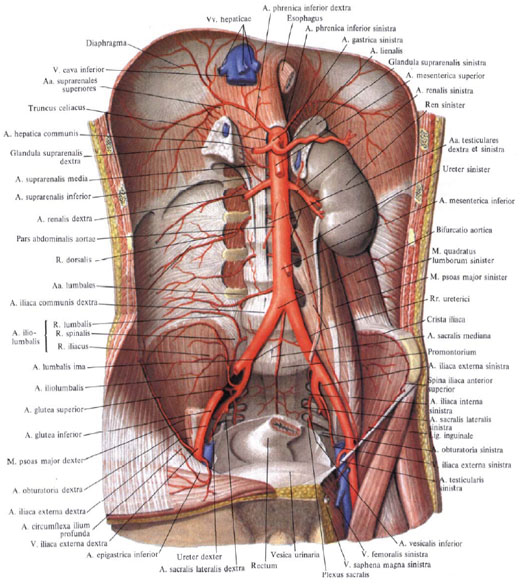
Abdominal aorta(abdominal aorta), pars abdominalis aortae (aorta abdominalis), is a continuation of the thoracic part of the aorta. It begins at the level of the XII thoracic vertebra and reaches the IV-V lumbar vertebra. Here the abdominal aorta divides into two common iliac arteries, aa. aliacae communes. The site of division is called the bifurcation of the aorta, bifurcatio aortica. A thin branch extends downwards from the bifurcation and lies on the anterior surface of the sacrum - the median sacral artery, a. sacralis mediana.
Two types of branches depart from the abdominal part of the aorta: parietal and splanchnic.
The abdominal part of the aorta is located retroperitoneally. In the upper part, the body of the pancreas and two veins adjoin its surface, crossing it: the splenic vein lying along the upper edge of the pancreas, v. lienalis, and left renal vein, v. renalis sinistra, running behind the gland. Below the body of the pancreas, in front of the aorta, is the lower part of the duodenum, and below it is the beginning of the root of the mesentery of the small intestine. To the right of the aorta lies the inferior vena cava, v. cava inferior; behind the initial section of the abdominal aorta there is a cistern of the thoracic duct, cisterna chyli, - the initial part of the thoracic duct, ductus thoracicus.
Parietal branches.
1. Inferior phrenic artery, a. phrenica inferior, is a rather powerful paired artery. It departs from the anterior surface of the initial part of the abdominal aorta at the level of the XII thoracic vertebra and goes to the lower surface of the tendon part of the diaphragm, where it gives off anterior and posterior branches that supply blood to the latter. In the thickness of the diaphragm, the right and left arteries anastomose with each other and with branches from the thoracic part of the aorta. The right artery passes behind the inferior vena cava, the left - behind the esophagus.
Along its course, the artery gives off 5 - 7 superior adrenal arteries, aa. suprarenales superiores. These are thin branches that arise from the initial section of the inferior phrenic artery and supply blood to the adrenal gland. Along the way, several small branches extend from them to the lower parts of the esophagus and to the peritoneum.
2. Lumbar arteries, aa. lumbales, are 4 paired arteries. They arise from the posterior wall of the abdominal aorta at the level of the body of the I-IV lumbar vertebrae. They are directed transversely, to the lateral side, with the two upper arteries passing behind the legs of the diaphragm, the two lower ones - behind the psoas major muscle.
All lumbar arteries anastomose with each other and with the superior and inferior epigastric arteries, which supply blood to the rectus abdominis muscle. Along their course, the arteries give a number of small branches to the subcutaneous tissue and skin; in the area of the white line they anastomose here and there with the arteries of the same name on the opposite side. In addition, the lumbar arteries anastomose with the intercostal arteries, aa. intercostales, iliopsoas artery, a. iliolumbalis, deep artery circumflexing the ilium, a. circumflexa ilium profunda, and the superior gluteal artery, a. glutea superior.
Having reached the transverse processes of the vertebrae, each lumbar artery gives off a dorsal branch, r. dorsalis. Then the lumbar artery goes behind the quadratus lumborum muscle and supplies it with blood; then it goes to the anterior wall of the abdomen, passes between the transverse and internal oblique abdominal muscles and reaches the rectus abdominis muscle.
The dorsal branch goes to the back surface of the body to the back muscles and skin of the lumbar region. Along the way, it gives off a small branch to the spinal cord - the spinal ramus, r. spinalis, which enters the spinal canal through the intervertebral foramen, supplying blood to the spinal cord and its membranes.

3. Median sacral artery, a. sacralis mediana, is a direct continuation of the abdominal aorta. It starts from its posterior surface, slightly above the bifurcation of the aorta, i.e. at the level of the V lumbar vertebra. It is a thin vessel passing from top to bottom in the middle of the pelvic surface of the sacrum and ending at the coccyx in the coccygeal body, glomus coccygeum.
Branching from the median sacral artery along its course are:
a) inferior lumbar artery, a. lumbalis imae, steam room, extends into the area of the V lumbar vertebra and supplies blood to the iliopsoas muscle. On its way, the artery gives off a dorsal branch, which is involved in the blood supply to the deep muscles of the back and spinal cord;
b) lateral sacral branches, rr. sacrales laterales, extend from the main trunk at the level of each vertebra and, branching on the anterior surface of the sacrum, anastomose with similar branches from the lateral sacral arteries (branches of the internal iliac arteries).
Several branches depart from the lower part of the median sacral artery, which supply blood to the lower parts of the rectum and the loose tissue around it.
Internal branches
I. Celiac trunk, truncus celiacus, is a short vessel, 1-2 cm long, extending from the anterior surface of the aorta at the level of the upper edge of the body of the 1st lumbar vertebra or the lower edge of the body of the 12th thoracic vertebra in the place where the abdominal aorta exits the aortic opening. The artery goes anteriorly and immediately divides into three branches: the left gastric artery, a. gastricasinistra, common hepatic artery, a. hepatica communis, and splenic artery, a. splenica (lienalis).

1. Left gastric artery, a. gastrica sinistra, the smaller of these three arteries. It rises slightly up and to the left; approaching the cardiac part, it gives off several branches towards the esophagus - esophageal branches, rr. esophageales, anastomosing with the branches of the same name from the thoracic part of the aorta, and itself descends to the right side along the lesser curvature of the stomach, anastomosing with the right gastric artery, a. gastrica dextra (from the common hepatic artery). On its way along the lesser curvature, the left gastric artery sends small branches to the anterior and posterior walls of the stomach.
2. Common hepatic artery, a. hepatica communis, is a more powerful branch, has a length of up to 4 cm. Moving away from the celiac trunk, it runs along the right leg of the diaphragm, the upper edge of the pancreas from left to right and enters the thickness of the lesser omentum, where it divides into two branches - the proper hepatic and gastroduodenal arteries.
1) Own hepatic artery, a. hepatica propria, moving away from the main trunk, goes to the gate of the liver in the thickness of the hepatoduodenal ligament, to the left of the common bile duct and somewhat anterior to the portal vein, v. portae. Approaching the gate of the liver, the proper hepatic artery divides into left and right branches, while the gallbladder artery departs from the right branch, a. cystica.
Right gastric artery, a. gastrica dextra, is a thin branch that arises from the proper hepatic artery, sometimes from the common hepatic artery. It is directed from top to bottom to the lesser curvature of the stomach, along which it runs from right to left, and anastomoses with a. gastrica sinistra. The right gastric artery gives off a number of branches that supply blood to the anterior and posterior walls of the stomach.
At the gate of the liver is the right branch, r. dexter, the proper hepatic artery sends the artery of the caudate lobe to the caudate lobe, a. lobi caudati, and arteries to the corresponding segments of the right lobe of the liver: to the anterior segment - the artery of the anterior segment, a. segmenti anterioris, and to the posterior segment - the artery of the posterior segment, a. segmenti posterioris.
Left branch, r. sinister, gives off the following arteries: artery of the caudate lobe, a. lobi caudati, and arteries of the medial and lateral segments of the left lobe of the liver, a. segmenti medialis et a. segmenti lateralis. In addition, a non-permanent intermediate branch, r, departs from the left branch (less often from the right branch). intermedius, which supplies the quadrate lobe of the liver.
2) Gastroduodenal artery, a. gastroduodenalis, is a rather powerful trunk. It is directed from the common hepatic artery downwards, behind the pyloric part of the stomach, crossing it from top to bottom. Sometimes the supraduodenal artery arises from this artery, a. supraduodenalis, which crosses the anterior surface of the head of the pancreas.
The following branches depart from the gastroduodenal artery:
a) posterior superior pancreaticoduodenal artery, a. pancreaticoduodenalis superior posterior, passes along the posterior surface of the head of the pancreas and, heading down, gives off pancreatic branches along its course, rr. pancreatici, and duodenal branches, rr. duodenales. At the lower edge of the horizontal part of the duodenum, the artery anastomoses with the inferior pancreaticoduodenal artery, a. pancreaticoduodenalis inferior (branch of the superior mesenteric artery, a. mesenterica superior);
b) anterior superior pancreaticoduodenal artery, a. pancreaticoduodenalis superior anterior, located in an arcuate manner on the anterior surface of the head of the pancreas and the medial edge of the descending part of the duodenum, directed downward, giving off duodenal branches along its path, rr. duodenales, and pancreatic branches, rr. pancreatici. At the lower edge of the horizontal part of the duodenum, it anastomoses with the inferior pancreaticoduodenal artery, a. pancreatoduodenalis inferior (branch of the superior mesenteric artery).
c) right gastroepiploic artery, a. gastroepiploica dextra, is a continuation of the gastroduodenal artery. It goes to the left along the greater curvature of the stomach between the leaves of the greater omentum, sends branches to the anterior and posterior walls of the stomach - gastric branches, rr. gastrici, as well as omental branches, rr. epiploici to the greater omentum. In the area of the greater curvature, it anastomoses with the left gastroepiploic artery, a. gastroepiploica sinistra (branch of the splenic artery, a. splenica);
d) retroduodenal arteries, aa. retroduodenales are the right terminal branches of the gastroduodenal artery. They surround the anterior surface of the right edge of the head of the pancreas.

3. Splenic artery, a. splenica, is the thickest of the branches extending from the celiac trunk. The artery goes to the left and, together with the vein of the same name, lies behind the upper edge of the pancreas. Having reached the tail of the pancreas, it enters the gastrosplenic ligament and splits into terminal branches heading to the spleen.
The splenic artery gives branches that supply blood to the pancreas, stomach and greater omentum.
1) Pancreatic branches, rr. pancreatici, extend from the splenic artery along its entire length and enter the parenchyma of the gland. They are represented by the following arteries:
a) dorsal pancreatic artery, a. pancreatica dorsalis, follows downwards according to the middle section of the posterior surface of the body of the pancreas and at its lower edge passes into the inferior pancreatic artery, a. pancreatica inferior, supplying blood to the lower surface of the pancreas;
b) large pancreatic artery, a. pancreatica magna, arises from the main trunk or from the dorsal pancreatic artery, follows to the right and runs along the posterior surface of the body and head of the pancreas. Connects to the anastomosis between the posterior superior and inferior pancreaticoduodenal arteries;
c) caudal pancreatic artery, a. caude pancreatis, is one of the terminal branches of the splenic artery, supplies blood to the tail of the pancreas.
2) Splenic branches, rr. splenici, 4 - 6 in total, are the terminal branches of the splenic artery and penetrate through the gate into the splenic parenchyma.
3) Short gastric arteries, aa. gastricae breves, in the form of 3-7 small stems, extend from the terminal section of the splenic artery and, in the thickness of the gastrosplenic ligament, go to the bottom of the stomach, anastomosing with other gastric arteries.
4) Left gastroepiploic artery, a. gastroepiploica sinistra, starts from the splenic artery at the place where the terminal branches depart from it to the spleen, and follows down in front of the pancreas. Having reached the greater curvature of the stomach, it moves along it from left to right, lying between the leaves of the greater omentum. At the border of the left and middle thirds of the greater curvature, it anastomoses with the right gastroepiploic artery (from A. gastroduodenalis). Along its course, the artery sends a number of branches to the anterior and posterior walls of the stomach - gastric branches, rr. gastrici, and to the greater omentum - omental branches, rr. epiploici.
5) Posterior gastric artery, a. gastrica posterior, non-permanent, supplies blood to the posterior wall of the stomach, closer to the cardiac part.
II. Superior mesenteric artery, a. mesenterica superior, is a large vessel that starts from the anterior surface of the aorta, slightly below (1 - 3 cm) the celiac trunk, behind the pancreas.

Coming out from under the lower edge of the gland, the superior mesenteric artery goes down and to the right. Together with the superior mesenteric vein located to the right of it, it runs along the anterior surface of the horizontal (ascending) part of the duodenum, crosses it across immediately to the right of the duodenojejunal flexure. Having reached the root of the mesentery of the small intestine, the superior mesenteric artery penetrates between the leaves of the latter, forming an arch convex to the left, and reaches the right iliac fossa.
Along its course, the superior mesenteric artery gives off the following branches: to the small intestine (with the exception of the upper part of the duodenum), to the cecum with the vermiform appendix, ascending and partially to the transverse colon.
The following arteries arise from the superior mesenteric artery.
1. Inferior pancreaticoduodenal artery, a. pancreaticoduodenalis inferior (sometimes not single), originates from the right edge of the initial section of the superior mesenteric artery. Divides into the anterior branch, r. anterior, and posterior branch, r. posterior, which go down and to the right along the anterior surface of the pancreas, bend around its head along the border with the duodenum. Gives branches to the pancreas and duodenum; anastomoses with the anterior and posterior superior pancreaticoduodenal arteries and with branches of a. gastroduodenalis.
2. Jejunal arteries, aa. jejunales, 7 - 8 in total, depart sequentially one after another from the convex part of the arch of the superior mesenteric artery, and are directed between the layers of the mesentery to the loops of the jejunum. On its way, each branch is divided into two trunks, which anastomose with the same trunks formed from the division of adjacent intestinal arteries.
3. Ileointestinal arteries, aa. ileales, in the amount of 5 - 6, like the previous ones, are directed to the loops of the ileum and, dividing into two trunks, anastomose with adjacent intestinal arteries. Such anastomoses of intestinal arteries have the form of arcs. New branches extend from these arcs, which also divide, forming arcs of the second order (slightly smaller in size). From the arches of the second order, arteries again depart, which, dividing, form arches of the third order, etc. From the last, most distal row of arches, straight branches extend directly to the walls of the loops of the small intestine. In addition to intestinal loops, these arches give rise to small branches that supply blood to the mesenteric lymph nodes.
4. Ileocolic artery, a. ileocolica, arises from the cranial half of the superior mesenteric artery. Heading to the right and down under the parietal peritoneum of the posterior wall of the abdominal cavity to the end of the ileum and to the cecum, the artery divides into branches supplying blood to the cecum, the beginning of the colon and the terminal ileum.
A number of branches arise from the ileocolic artery:
a) the ascending artery goes to the right to the ascending colon, rises along its medial edge and anastomoses (forms an arch) with the right colon artery, a. Colica dextra. The colonic branches extend from this arch, rr. colici, supplying blood to the ascending colon and the upper part of the cecum;
b) anterior and posterior cecal arteries, aa. cecales anterior et posterior, are directed to the corresponding surfaces of the cecum. Are a continuation of a. ileocolica, approach the ileocecal angle, where, connecting with the terminal branches of the ileointestinal arteries, they form an arch, from which branches extend to the cecum and to the terminal ileum - ileointestinal branches, rr. ileales;
c) arteries of the appendix, aa. appendiculares, arise from the posterior caecum artery between the layers of the mesentery of the appendix; supply blood to the vermiform appendix.
5. Right colonic artery. a. colica dextra, departs from the right side of the superior mesenteric artery, in its upper third, at the level of the root of the mesentery of the transverse colon, and goes almost transversely to the right, to the medial edge of the ascending colon. Before reaching the ascending colon, it is divided into ascending and descending branches. The descending branch connects to branch a. ileocolica, and the ascending branch anastomoses with the right branch of a. Colica media. From the arches formed by these anastomoses branches extend to the wall of the ascending colon, to the right flexure of the colon and to the transverse colon.

6. Middle colonic artery, a. colica media, departs from the initial section of the superior mesenteric artery, goes forward and to the right between the leaves of the mesentery of the transverse colon and is divided at the bottom of the branch: right and left.
The right branch connects to the ascending branch a. colica dextra, and the left branch runs along the mesenteric edge of the transverse colon and anastomoses with the ascending branch of a. colica sinistra, which arises from the inferior mesenteric artery. Connecting in this way with the branches of neighboring arteries, the middle colonic artery forms arches. From the branches of these arches, arches of the second and third order are formed, which give direct branches to the walls of the transverse colon, to the right and left bends of the colon.
III. Inferior mesenteric artery, a. mesenterica inferior, originates from the anterior surface of the abdominal aorta at the level of the lower edge of the third lumbar vertebra. The artery runs retroperitoneally to the left and down and divides into three branches.

1. Left colic artery, a. colica sinistra, lies retroperitoneally in the left mesenteric sinus in front of the left ureter and the left testicular (ovarian) artery, a. testicularis (ovarica) sinistra; is divided into ascending and descending branches. The ascending branch anastomoses with the left branch of the middle colic artery, forming an arch; supplies blood to the left part of the transverse colon and the left flexure of the colon. The descending branch joins the sigmoid artery and supplies the descending colon.
2. Sigmoid-colic artery, a. sigmoidea (sometimes there are several of them), goes down first retroperitoneally, and then between the layers of the mesentery of the sigmoid colon; anastomoses with the branches of the left colic artery and the superior rectal artery, forming arches from which branches supplying the sigmoid colon arise.
3. Superior rectal artery, a. rectalis superior, is the terminal branch of the inferior mesenteric artery; heading down, it divides into two branches. One branch anastomoses with the branch of the sigmoid artery and supplies the lower parts of the sigmoid colon. The other branch goes to the pelvic cavity and crosses a. iliaca communis sinistra and, lying in the mesentery of the pelvic part of the sigmoid colon, is divided into right and left branches that supply blood to the ampulla of the rectum. In the intestinal wall they anastomose with the middle rectal artery, a. rectalis media, branch of the internal iliac artery, a. iliaca interna.
IV. Middle adrenal artery, a. suprarenalis media, steam room, extends from the side wall of the upper aorta, slightly below the origin of the mesenteric artery. It is directed transversely outward, crosses the crus of the diaphragm and approaches the adrenal gland, in the parenchyma of which it anastomoses with the branches of the superior and inferior adrenal arteries.
V. Renal artery, a. renalis, - paired large artery. It starts from the lateral wall of the aorta at the level of the second lumbar vertebra, almost at a right angle to the aorta, 1-2 cm below the origin of the superior mesenteric artery. The right renal artery is slightly longer than the left, since the aorta lies to the left of the midline; heading towards the kidney, it is located behind the inferior vena cava.
Before reaching the hilum of the kidney, each renal artery gives off a small inferior adrenal artery, a. suprarenalis inferior, which, having penetrated the adrenal parenchyma, anastomoses with the branches of the middle and superior adrenal arteries.
In the region of the renal hilum, the renal artery divides into anterior and posterior branches.
Anterior branch, r. anterior, enters the renal gate, passing in front of the renal pelvis, and branches, sending arteries to the four segments of the kidneys: the artery of the upper segment, a. segmenti superioris, - to the upper; artery of the upper anterior segment, a. segmenti anterior superioris, - to the upper anterior; artery of the lower anterior segment, a. segmenti anterior is inferioris, - to the lower anterior and artery of the lower segment, a. segmenti inferioris, - to the lower. Posterior branch, r. posterior, the renal artery passes behind the renal pelvis and, heading to the posterior segment, gives off the ureteric branch, r. uretericus, which can arise from the renal artery itself, is divided into posterior and anterior branches.
VI. Testicular artery, a. testicularis, paired, thin, departs (sometimes right and left by a common trunk) from the anterior surface of the abdominal aorta, slightly below the renal artery. It goes down and laterally, runs along the psoas major muscle, crosses the ureter on its way, and above the arcuate line - the external iliac artery. Along the way, it gives branches to the fatty capsule of the kidney and to the ureter - ureteric branches, rr. ureterici. Next it goes to the deep inguinal ring and, here joining the vas deferens, passes through the inguinal canal into the scrotum and breaks up into a number of small branches going into the parenchyma of the testicle and its epididymis - branches of the epididymis, rr. epididymales.
Along its course it anastomoses with a. cremasterica (branch of a. epigastrica inferior and with a. ductus deferentis (branch of a. iliaca interna).
In women, the corresponding testicular artery is the ovarian artery, a. ovarica, gives off a number of ureteral branches, rr. ureterici, and then passes between the leaves of the broad ligament of the uterus, along its free edge, and gives off branches to the fallopian tube - tubal branches, rr. tubales, and into the gate of the ovary. The terminal branch of the ovarian artery anastomoses with the ovarian branch of the uterine artery.
Thrombosis of the mesenteric artery is a violation of blood circulation in the mesenteric vessels. This condition is the cause of acute intestinal ischemia in 25% of cases. The pathology is expressed in severe pain in the lower abdomen, which is accompanied by bloody impurities, as well as shock. To help the patient, he needs to undergo emergency surgery.
The superior mesenteric artery is responsible for supplying blood to the small intestine, cecum, ascending colon, and transverse colon. Part of the transverse colon, the entire colon, sigmoid colon and rectum receive nutrition from the inferior mesenteric artery. Most often, the superior mesenteric artery, which is responsible for the blood supply to the digestive tract as a whole, is affected. However, mixed lesions of the mesenteric veins and arteries cannot be excluded. First, a thrombus clogs the lumen of one vessel, and then chronic obstruction of another vessel develops. The pathology most often affects men over 50 years of age.
Until now, thrombosis of the mesenteric artery remains a pressing problem for surgeons. This is explained not only by the difficulties in diagnosing the pathological condition, but also by the fact that it can be caused by many reasons and often leads to the death of the patient.

Thrombosis of the mesenteric artery can be due to several reasons, including:
Previous operations on the cardiac aorta.
The presence in the body of a tumor of a malignant nature.
Blood hypercoagulation, polycythemia vera, thrombocytosis, sickle cell anemia.
The period of bearing a child.
Taking hormonal drugs for the purpose of contraception.
Paraneoplastic syndrome.
Infection of organs located in the peritoneal cavity, including diverticulitis, appendicitis, etc.
Liver cirrhosis with portal hypertension leading to venous stasis.
Surgical intervention accompanied by injury to the mesenteric artery.
Anastomosis.
Decompensated disease.
Thrombosis occurs when the mesenteric artery is blocked by thrombotic masses. As a result, blood flow slows down, which leads to pathological changes in the organ.
There are three possible development options for this pathological condition. In the first case, blood flow can be restored spontaneously or with the help of medications (thrombosis with compensation of blood flow in the mesenteric artery). In this case, the functioning of the intestines will not be impaired.
In the second case, impaired blood flow will lead to various intestinal diseases (thrombosis with subcompensation of blood flow in the mesenteric artery).
In the third case, impaired blood flow causes purulent peritonitis, sepsis and death of the patient (decompensated type thrombosis).
Elderly people.
Patients with malignant tumors of the peritoneum.
Patients undergoing atrial fibrillation.

Acute thrombosis of the mesenteric artery has a sudden onset. Severe pain comes to the fore. They are localized in the abdomen and proceed like contractions. A person is unable to stay in one place; he constantly rushes about in search of a comfortable body position that will relieve pain. The patient feels best when the knees are pressed tightly to the stomach.
Other signs of mesenteric artery thrombosis:
The patient feels nauseous and may vomit. Bile and blood are found in the vomit. Then the vomit will start to smell like feces.
The stool is liquid and blood is visible in it.
The skin of the face and body becomes cyanotic.
Shock may develop.
After 6-12 hours from the onset of the pathological process, the pain becomes less intense. At the same time, it acquires a more precise localization, that is, it does not spread throughout the peritoneum, but is concentrated in the intestinal area.
In the area between the navel and pubis, you can feel a tumor-like compaction.
The patient’s health is getting worse: the pulse quickens, but the blood pressure returns to normal.
After 18-36 hours from the start of the first symptoms, the patient develops peritonitis. His condition deteriorates sharply, the pain becomes incredibly intense, especially during physical activity. Signs of intoxication of the body are increasing.
The patient cannot empty the intestines, as paralytic obstruction develops.
So, in its development, thrombosis of the mesenteric artery goes through three phases: a hyperactive phase (the first 6-12 hours), a paralytic phase (12-18 hours) and shock (18-36 hours).

During an examination of a patient who was admitted to a medical facility in the first hours after the onset of thrombosis, the doctor will discover a soft abdomen and the participation of the peritoneal wall in breathing. There are no symptoms of internal irritation of the peritoneum, that is, the severity of the pathology does not correspond to the initial symptoms of the disease. This is one of the factors that complicates making a correct diagnosis. An increase in body temperature and signs of irritation of the peritoneum will appear only at the stage of peritonitis, when it will be difficult to help the patient.
It is imperative to check with the patient whether he has previously had an attack of angina with abdominal pain that would occur after eating. As a rule, about 50% of patients with mesenteric artery thrombosis give a positive answer to this question. Since the process of digesting food increases intestinal perfusion, the patient may suffer from exhaustion, since such patients often develop fear of eating, and satiety occurs much faster.
Conditions in the medical history such as ischemic heart disease, atherosclerosis, obliterating endarteritis, as well as surgical interventions on the aorta may suggest thrombosis of the mesenteric artery.
What to pay attention to:
As intestinal necrosis develops, the pain may subside somewhat. Patients take this as a trend towards improvement, which is a false belief.
Narcotic painkillers do not reduce the intensity of painful sensations. At the beginning of the development of thrombosis symptoms, antispasmodics are much more effective.
As the disease progresses, intoxication of the body increases.
Symptoms of thrombosis most often do not correspond to the severity of ischemic intestinal damage.
To perform a high-quality diagnosis, it is necessary to perform the following studies:
X-ray of the intestines. You should pay attention to such indicators as: excessive distension of the intestine, its thickened wall, etc. The specificity of the method does not exceed 30%.
CT scan of the intestines. Signs of mesenteric artery thrombosis: swelling of the intestinal wall, hemorrhages in certain areas of the intestine. This method allows visualization of the thrombus. However, CT with vascular angiography has greater specificity. This study can detect thrombosis in 94% of cases.
Angiography of intestinal vessels. Allows you to make a correct diagnosis in 88% of cases.
USGD has specificity in 92-100% of cases. However, if the thrombus is located outside the great vessels, then the study will not detect it. Therefore, this method is not taken as a basis, it is regarded as auxiliary.
Other methods that allow you to clarify the diagnosis: MRI (disadvantages: expensive research, lack of necessary equipment in many clinics, but the method is highly specific), echocardiography (makes it possible to clarify the source of the blood clot), ECG, etc.
The patient's blood must be taken for biochemical and general analysis, as well as for a coagulogram.

After admission to the hospital, the patient is placed in the intensive care unit.
The following treatment is indicated for him:
Restoring the water-salt balance of the body.
Correction of electrolyte levels.
Oxygen therapy.
If there are indications, the patient is given a blood transfusion.
Monitoring blood pressure and diuresis.
Placement of a nasogastric tube.
Normalization of the heart muscle.
Pain relief.
Prescription of broad-spectrum antibacterial drugs.
Use of medicines:
Administration of Papaverine through a catheter into the affected area of the intestine. The drug is administered throughout the day (this is the minimum period for administering the drug). You cannot combine the use of Papaverine and Heparin.
Administration of trobolytics via catheter, provided that the patient has not yet developed peritonitis or intestinal necrosis. It is important to perform this procedure no later than 8 hours from the onset of symptoms. If after 4 hours the patient’s well-being does not improve, then surgery is recommended.
Introduction of Heparin followed by transition to Warfarin.
Surgery:
Intestinal resection is prescribed if the patient develops peritonitis.
Revascularization with further anastomosis can also be considered as a method of surgical treatment for mesenteric artery thrombosis.
According to various authors, the death rate of patients with mesenteric thrombosis can reach 50-100%. A more accurate prognosis depends on the speed of seeking medical help. It is aggravated by the fact that many patients go to the doctor with already developed or peritonitis. If the patient refuses surgery, then death occurs in 100% of cases.
Prevention of mesenteric artery thrombosis
Prevention of mesenteric artery thrombosis comes down to maintaining a healthy lifestyle and quitting smoking. It is also important to monitor your body weight to prevent obesity.
It is imperative to treat all diseases that pose a threat to the formation of a blood clot. We are talking about atherosclerosis, rheumatism, arrhythmia, etc.
Education: Moscow State Medical and Dental University (1996). In 2003, he received a diploma from the educational and scientific medical center for the administration of the President of the Russian Federation.
Embolism of the superior mesenteric artery manifests itself as an acute onset of intense abdominal pain, usually localized in the umbilical region, but sometimes in the right lower quadrant of the abdomen. The intensity of pain often does not correspond to the data obtained from an objective examination of such patients. The abdomen remains soft upon palpation, or there is only slight soreness and tension in the muscles of the anterior abdominal wall. Intestinal peristalsis is often heard. Patients with superior mesenteric artery embolism often experience nausea, vomiting, and often diarrhea. In the early stages of the disease, stool examination reveals a positive reaction to occult blood, although, as a rule, there is not a large amount of blood in the stool.
A careful history of the disease can suggest the cause of the embolism. Classically, such patients always have signs of diseases of the cardiovascular system, most often atrial fibrillation, recent myocardial infarction or rheumatic lesions of the heart valves. A careful history often reveals that patients have previously had episodes of embolism, both in the form of strokes and peripheral arterial embolism. Angiography can identify the following emboli localization options:
Mouth (5.2%)
– the blood supply to the entire small intestine and the right half of the colon is disrupted
I segment (64.5%) – the embolus is localized to the origin of the a.colica media
– as well as when the embolus is localized at the mouth of the superior mesenteric artery, the blood supply to the entire small intestine and the right half of the colon is disrupted
II segment (27.6%) – the embolus is localized in the area between the points of origin of a.colica media and a.ileocolica
– the blood supply to the ileum and ascending colon to the hepatic flexure is disrupted
III segment (7.9%) – the embolus is localized in the area below the origin of the a.ileocolica
– blood supply to the ileum is disrupted
Combination of segment I embolism with occlusion of the inferior mesenteric artery
– blood supply to the entire small and large intestine is disrupted
Treatment. A large number of conservative treatments have been proposed for the treatment of superior mesenteric artery embolism. Although conservative treatment methods are sometimes successful in patients with acute embolism of the superior mesenteric artery, the best results are observed with surgical intervention. After laparotomy, the superior mesenteric artery is usually opened in a transverse direction at its origin from the aorta behind the pancreas. An embolectomy is performed, and once blood flow is restored through the superior mesenteric artery, the small bowel is carefully examined to determine its viability. To identify irreversible ischemic changes in the intestinal wall, a fairly large number of different tests have been proposed. Most often, a routine examination of the intestine is performed, which is often quite sufficient. The final conclusion about the condition of the intestinal wall is made after the intestine is warmed for 30 minutes either by lowering it into the abdominal cavity or by covering it with napkins moistened with warm saline solution. If there are signs of necrosis, intestinal resection is performed with end-to-end interintestinal anastomosis using a stapler. After the operation, the patient is sent to the intensive care unit. Sometimes, in patients who have undergone intestinal resection due to its necrosis due to acute embolism of the superior mesenteric artery, a second operation is performed after 24 hours, the so-called in order to examine the anastomosed edges of the intestine and ensure their viability. During the first operation, some surgeons prefer not to perform an interintestinal anastomosis, but suture both ends of the intestine using staplers. During reoperation, if a viable intestine is present, an interintestinal anastomosis is performed.
There are several reasons for the relatively high mortality rate after embolectomy from the superior mesenteric artery. Such patients often have very severe cardiovascular diseases that do not allow them to undergo major surgical interventions. Sometimes the diagnosis of embolism of the superior mesenteric artery is made late, which leads to the development of extensive intestinal necrosis. Systemic purulent-septic complications and enteral insufficiency due to resection of a large section of intestine also aggravate the condition of patients and often lead to death.
- Superior mesenteric artery, a mesenterial superior. Unpaired branch of the abdominal aorta. It begins approximately 1 cm below the celiac trunk, first lies behind the pancreas, then passes in front of the uncinate process. Its branches continue into the mesentery of the small and transverse colon. Rice. A, B.
- Inferior pancreaticoduodenal artery pancreaticoduodenalis inferior. It arises at the level of the upper edge of the horizontal part of the duodenum. Its branches lie in front and behind the head of the pancreas. Rice. A. 2a Anterior branch, ramus anterior. Anastomoses with the anterior superior pancreaticoduodenal artery. Rice. IN.
- Jejunal arteries, aajejunales. Goes to the jejunum in its mesentery. Rice. A.
- Ileal arteries, aa ileales. They approach the ileum between the two layers of its mesentery. Rice. A.
- Ileocolic artery, a. ileocolica. In the mesentery of the small intestine it goes down and to the right to the iliocecal angle. Rice. A.
- Colon branch, ramus colicus. It goes to the ascending colon. Anastomoses with the right colonic artery. Rice. A.
- Anterior cecal artery, a. caecalis (cecalis) anterior. In the cecal fold it approaches the anterior surface of the cecum. Rice. A.
- Posterior cecal artery, a. caecalis (cecalis) posterior. It goes behind the final section of the ileum to the posterior surface of the cecum. Rice. A.
- Artery of the vermiform appendix, a. appendicularis. It crosses the ileum posteriorly and lies along the free edge of the mesentery of the appendix. The origin of the artery is not constant; it can be double. Rice. A. 9a Ileal branch, ramus ile: alis. It goes to the ileum and anastomoses with one of the small intestinal arteries. Rice. A.
- Right colic artery, a. Colica dextra. Anastomoses with the ascending branch of the ileocolic and middle colic arteries. Rice. A. 10a Artery of the right flexure of the colon, aflexura dextra. Rice. A.
- Middle colic artery, a. Colica media. Located in the mesentery of the transverse colon. Rice. A. Pa Marginal colic artery, a. marginalis coli []. Anastomosis of the left colon and sigmoid arteries. Rice. B.
- The inferior mesenteric artery, and tesenterica inferior. Departs from the abdominal aorta at the level of L3 - L4. It goes to the left and supplies the left third of the transverse colon, descending, sigmoid colon, as well as most of the rectum. Rice. B. 12a Ascending [intermesenteric] artery, a ascendeus. Anastomoses with the left colic and middle colic arteries. Rice. A, B.
- Left colic artery, a. Colica sinistra. Retroperitoneally directed to the descending colon. Rice. B.
- Sigmoid intestinal arteries, aa. sigmoideae. It goes obliquely down to the wall of the sigmoid colon. Rice. B.
- Superior rectal artery, a. rectalis superior. Behind the rectum it enters the small pelvis, where it divides into right and left branches, which, perforating the muscle layer, supply blood to the intestinal mucosa to the anal valves. Rice. B.
- The middle adrenal artery, and suprarenalis (adrenalis) media. It arises from the abdominal aorta and supplies blood to the adrenal gland. Rice. IN.
- Renal artery, a. renalis. It starts from the aorta at level L 1 and is divided into several branches that go to the gate of the kidney. Rice. B, D. 17a Capsular arteries, aaxapsulares (perirenales). Rice. IN.
- Inferior adrenal artery, a. suprarenalis inferior. Participates in the blood supply to the adrenal gland. Rice. IN.
- Anterior branch, ramus anterior. Supplies blood to the upper, anterior and lower segments of the kidney. Rice. V, G.
- Artery of the upper segment, a. segment superioris. Spreads to the posterior surface of the kidney. Rice. IN.
- Artery of the upper anterior segment, a.segmenti anterioris superioris. Rice. IN.
- Artery of the lower anterior segment, a segmenti anterioris inferioris. Branch to the anterioinferior segment of the kidney. Rice. IN.
- Artery of the lower segment, a. segmenti inferioris. Spreads to the posterior surface of the organ. Rice. IN.
- Posterior branch, ramus posterior. It goes to the posterior, largest segment of the kidney. Rice. V, G.
- Artery of the posterior segment, a. segmenti posterioris. Branches in the corresponding segment of the kidney. Rice. G.
- Ureteral branches, rami ureterici. Branches to the ureter. Rice. IN.
