The cerebral cortex, its connection with the spinal cord. Nervous system. Brain and nerves
You have had an accident or suffered an illness that unfortunately resulted in spinal cord injury or damage (SCI). In this section, we will begin to explain how your body functions and how its functioning is affected by PSM, which varies from case to case. You may experience only part of its consequences or the full range of its influence. This book will serve as a launching pad, awaken the desire to receive new information and lead to new questions. Talk to the professionals who care about you about what you think is important here.
What does the term spinal cord injury mean?
Spinal cord injury occurs when damage to the spinal cord interrupts the connection between the brain and the body. If it is caused by physical force and is expressed in the divergence, rupture, cut or crushing of the spinal cord, then it is called traumatic injury . It may occur due to one of the most common four types of vertebral fractures, which are visible in the pictures.
The spinal cord can also become damaged as a result of multiple sclerosis or tumor growth.
Although spinal cord injury refers to damage to nerve tissue, it is more easily characterized by the level of injury to the bony part of the spine. The affected area of the spinal cord is more accurately identified by vertebral numbers. This is why the level of your injury is called by two or more vertebrae, for example, “tetraplegia at the C5/6 level.”
“The last thing I remember is how I climbed onto the ATV to turn around. We stopped to admire the view from the highest point of Whanganui Farm. It was a hot, sunny February day (this took place in the Southern Hemisphere - L.I.). I did not pay attention or simply did not see the red indicator light that indicated that the motorcycle was parked in the “reverse” position. I don’t remember myself, but they later told me that the motorcycle jerked back and fell off a steep cliff. Then I seemed to be conscious, but nothing came to my mind except strange, dream-like memories, until two weeks later I found myself lying on my back in a small ambulance plane.”
Ian Popeye, T5
First aid. Surgical intervention
To immobilize a damaged spine, you may need surgical intervention. The spine may become unstable, become significantly deformed, or may partially compress the spinal cord. Metal plates and anchors are often used to stabilize and prevent further injury to the spinal cord. Keep in mind that stabilization surgery only restores the bony part of the spine, not the spinal cord.
Spinal stabilization
Regardless of the nature of the spinal injury, he will need immobility for some time. If the cervical part of the spine is damaged, it is possible that you will be forced to lie on your back in traction, with devices attached to the protrusions of the skull. This will help keep the vertebrae in a stable position while fusion occurs. This traction usually takes about six weeks.
For other damage cervical region To keep the spine motionless, you may need to wear a special neck ring or a so-called Halo vest.
“If you are already in a spinal cord injury unit, listen to all the advice. His amazing staff are too busy, they are simply crushed by the burden of responsibilities, therefore, when expressing your requests, be patient - sometimes you need to wait a little until you get an answer to your question. Save your energy for more important things."
Roy Dale, L4/5 injury.
Immediate consequences of injury
In paralyzed parts of the body you will not feel excessive compression, and with immobilized limbs you will not be able to relieve it. Therefore, in order to reduce pressure on the tissue and avoid the development of bedsores, you should change your body position every two to three hours, and you will have to turn over.
You will not feel your bladder full and will not be able to empty it. Until you yourself learn to manage its work, your attending physician or nurse will do this.
To free your rectum first, you will also need the help of staff.
Since you yourself will not be able to move your paralyzed limbs, in order to avoid their deformation and the development of contractures, they will be handled by a specialist in physical therapy.
You may experience spasticity - uncontrollable muscle tension or limb twitching.
Women may notice that their periods will stop for a while or appear earlier or later than expected.
Men find that their erections have disappeared or that they are unable to keep them.
If you are a tetraplegic - a “collar”, your body’s thermoregulation system may be impaired. The temperature will be significantly lower than normal, and you will shiver from the cold or, on the contrary, feel hot, but you will not sweat.
You will not be able to sit straight without support, and at the very beginning you will generally need to be raised into a sitting position, and gradually and a short time. If you are lifted too quickly, especially with a high level of spinal cord damage, you may lose consciousness altogether.
In the first weeks you may suffer from very low blood pressure, and after about a month you may experience blood pressure spikes.
Being in sitting position, you will understand that you will not be able to maintain your balance without outside help. You will have to learn this again, relying on sensations and controlling the extreme inclinations.
You may become deeply depressed or alternate between anger and guilt. This is a completely natural reaction to trauma, to shock, to the monotony of lying on your back in the hospital, to humiliating inaction, to the uncertainty of your future, to worry about family and friends.
For several months you will not be able to return home, start work and study, have sex, care for children, take care of older family members, play sports and cook food. But believe that after some preparation, most of the things that you took for granted in everyday life before the injury will be available to you. Over time, you will be able to do everything or almost everything you did before. And although life in general will be more difficult, you will experience much greater pleasure from the results of your activities.
Some paraplegics (“spinal patients”) will be able to be discharged home after a month and a half, and tetraplegics (“collar patients”) after four months, but for the majority this period will last longer - from 4 to 12 months.
A few words about medical terms
Medical science has evolved over the centuries. Many of its terms are based on Latin. The language of medicine was designed to be precise and clearly defined, leaving no room for ambiguity among practitioners. Some terms may seem impersonal, harsh, or even negative to you.
Disabled, non-functional, incomplete, lethargic, defeat and others - all these terms describe different aspects of your condition. Remember: you are a human person who, by chance, received some bodily injuries. Don't let yourself be described using "medical jargon"! If you do not understand medical terminology, calmly ask someone who uses it in a conversation with you to explain the words you do not understand.
Material borrowed from the book
"Striving Forward: How to Live with Spinal Cord Damage."
Spinal cord lesion
Association of Persons with Spinal Cord Injury (SCI),
UK, May 1995.
Get to know your spine
Spine- is a pillar consisting of bones, ligaments and nerves and performs the two most important roles. Firstly, it is the physical structure that connects most parts of the body, and secondly, it houses the spinal cord, which connects the brain to every part of the body. The spine starts from the neck and ends at the tailbone. The spine is a column made up of 33 individual bones, each called a vertebra.

The vertebrae are located one on top of the other and are held together by intervertebral discs, ligaments and muscles. Ligaments support the spine in a stable position, and muscles provide movements limited to a certain amplitude.
Elastic discs between every two vertebrae prevent the surfaces of the bones from rubbing against each other and act as shock absorbers for everything. spinal column.
The spine is divided into 4 parts (divisions). Each of the departments has its own name, and each vertebra has its own number.

Peripheral nerves and their functions
A pair of nerves emerge from each vertebra, and there are eight of them in the cervical region, i.e. one pair more than the vertebrae themselves. There is a hole in the center of each vertebra, and when the vertebrae are connected, a single passage is formed between them, called the spinal canal. It surrounds the spinal cord and completely protects it.
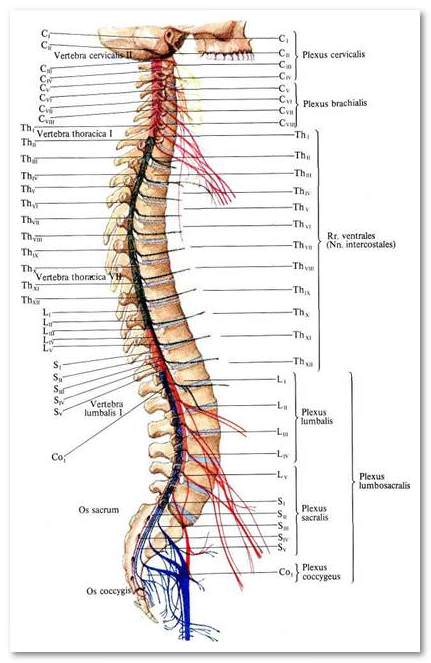
Pairs of peripheral nerves leave the spinal cord through the gaps between the vertebrae. Each pair connects the spinal cord to different parts of the body. The figure below shows which part of the body each pair of peripheral nerves goes to.

Your nervous system
The nervous system consists of the brain, the spinal cord and the nerves that come from it. The brain controls all activities of the body. Some body functions are controlled automatically by the brain, such as heartbeat and breathing, which we are not even aware of. Other functions are performed consciously, after making a volitional decision, for example, picking up an object from the floor.
Your nervous system helps control all body functions and can roughly be divided into two parts. The brain and spinal cord make up central nervous system, A peripheral nervous system connects the central nervous system to other parts of the body. According to principle functional organization the entire nervous system can also be divided into two subsystems - somatic And autonomic nervous systems.

Somatic nervous system
The somatic nervous system is the main mode of communication between the brain and the moving parts of the body. Its main significance is to transmit excitation to the brain and, after this information is processed in it and a response is established, to control voluntary movements. The following are some of the functions that are checked and controlled by the somatic nervous system:
· Movement
Sensitivity
· Reflexes
Autonomic nervous system
The autonomic nervous system controls the unconscious or automatic functions of the glands and internal organs. When the spinal cord is damaged, the autonomic nervous system is usually also damaged. The following are the functions that are checked and controlled by the autonomic nervous system:
· Heart rate and blood pressure.
· Breathing.
· Body temperature.
· Sweating.
· Trembling.
· Digestion.
· Functions of the rectum and bladder.
· Functions of male genital organs.
Your spinal cord
Is yours spinal cord is a very complex two-way communication network that allows the brain to “communicate” with specific areas of the body, and these areas to send response impulses to the brain. The spinal cord is like a telephone cord with many wires. The spinal cord is as thick as a little finger, descends along the spinal canal from the brain and ends at the level of L1 - the first lumbar vertebra. At this point the spinal cord branches into a bundle of nerves called ponytail .
The spinal cord has three protective spheres.
1. The most external of them dura mater is the most durable.
2. Medium arachnoid as if woven from a spider's web.
3.Pia mater very thin, but it provides waterproof insulation and keeps the brain tissue in the very center. It is called spinal tissue. It cushions and protects the spinal cord and spine from shock and damage.

The spinal cord itself in cross-section has the shape of a butterfly with two clearly defined zones - gray matter And white matter. The most important function of the spinal cord is to transmit messages from your body to the brain and from the brain to different parts of the body.
“I was injured in 1995 at Cave Creek when an observation deck collapsed and 18 people fell from a 35-meter cliff onto sharp rocks. I was one of four survivors. Fortunately, I do not remember either the accident itself or half of the entire time spent in resuscitation. In addition to incomplete tetraplegia C6/7, I broke 16 bones, including my lower jaw in three places, I had a rupture of the rectum and damage to the skull. I spent a year in the spinal cord injury unit at Barwood with the intention of doing more rehab, but it actually only started when I got back into real life."
Steve Hannen
Neural connections and signals
These messages or signals travel along pathways in the white matter of the spinal cord. Like an escalator, these paths have a clearly defined direction of movement. Some are designed to transmit messages to the brain, others in the opposite direction.

The three different types of messages that travel along the spinal cord are:
1. SENSITIVITY OR SENSORY SIGNALS.
2. MOTOR OR MOTOR SIGNALS.
3. PROTECTIVE SIGNALS OR REFLEXES.
Sensory signals
Sensory signals are sent to the spinal cord from different parts of the body, say from the hand. The spinal cord then sends them to the brain. When they reach the brain, they are perceived as sensitivity, i.e. touch, pain, high or low temperature.
There is one more vital important feeling, which you had no idea about before. In Latin it is called proprioception . It subconsciously informs you about the position of your limbs and joints. Proprioceptive signals tell the brain about the body's position so that the brain can accurately coordinate unconscious movements, such as when it's time to change the position of the hand.
Motor signals
Motor messages are generated in the brain and transmitted along the spinal cord. The spinal nerves send messages to the appropriate parts of the body, and these signals control the functioning of most muscles.

1. Pain signal from the leg. 2. A reflex reaction missed by the spinal cord. 3. The brain becomes convinced that panic is groundless and stops reflex movements.
Reflex signals
Your body has an amazing defense mechanism built into it. It turns out that not all messages are from different parts bodies go all the way to the brain. The spinal cord is capable of making independent decisions in this regard. For example, if you step on a button, the skin sends a sensory message about this. If this message is perceived as a panic signal, the spinal cord will send a reflex signal to the muscle group where it originated, and the leg will immediately withdraw from this source pain, without making you think, i.e. this will happen automatically. But the initial message will still reach the brain, and it will limit the strength of the reflex response to slow down the movement of the leg.
What happened to my nervous system
Motor signals cannot pass through the injured area, so the brain cannot control muscles below the level of injury. In the same way, sensory signals do not pass from below and do not reach the brain, so you do not feel heat or cold, pain or pressure. Ask your doctor to show you in this diagram where the affected part of your spinal cord is located.
Reflex signals may still loop or bounce off the spinal cord, but the brain is no longer able to suppress reflex movements. This leads to muscle spasms, spasticity or "spasticity" . Remember that the motor, sensory and reflex signals, once started between the brain and the body, will never stop, they simply will not overcome the level of your trauma.
Damage to the spinal cord does not prevent the muscles located below the level of injury from receiving blood and nutrition. After an injury, you may experience changes in your breathing, temperature, heart rate and blood pressure. Most likely, you will also feel changes in the functioning of the rectum, bladder and genitals. For a new patient, there will be great anxiety about not knowing how the injury will affect one's sex life and ability to have children. This topic is discussed in more detail in a separate chapter below.

Spinal shock
Immediately after the injury, the spinal cord may be in a state of shock. During this time, reflexes, movement, and sensation below the level of injury may be absent. Spinal shock can last for several hours in some people, and in others for several months. It is because of shock in the early stages after injury that we cannot accurately determine which body functions are lost. It may be a few weeks after the shock ends that you may begin to feel some movement or sensation restored, but this will vary from person to person.
Restoration of any form of reflex activity below the level of injury indicates recovery from the state of spinal shock.
Reflexes and spasticity
Before injury reflex activity was a normal function of the spinal cord. This system urgent action protects the body and prevents self-injury, such as keeping it away from heat sources.
Painful squeezing of muscles or painful sensations of the skin cause the appearance of sensory signals emanating from nerve endings on this area of the body. Weak signals travel first to the spinal cord and then to the brain. Stronger signals are reflected directly from the spinal cord back to the muscles, which makes it possible to remove an area of the body from the source of pain or discomfort. The brain controls the defense reflex by limiting the response to a single movement of moderate force.
If your spinal cord is damaged at T12 or higher, your protective reflexes are likely intact and still active. Signals from the spinal cord directly to the muscles are still reflected, but the brain cannot dampen or control muscle movements. In this situation, muscle spasm occurs. For injuries at level T12 and below, this spasticity usually doesn't happen.
You probably cannot imagine that “spasticity” can be a positive phenomenon, but, take my word for it, it can bring considerable benefits to spinal patients. So, spasticity indicates that something is wrong with you. After a while you will learn to distinguish different types spasticity as signals that will indicate exactly what has happened, for example, the filling of the bladder. Spasticity also keeps the muscles of the limbs toned, promotes blood circulation and helps the bladder and intestines work.
For example, a full bladder will try to send sensory signals to the brain that it needs to be emptied. This message will not reach the brain, but it will excite a reflex signal from the spinal cord, which will command the bladder muscles to empty.
“I was at home and while cleaning the windows, I fell from the roof of the carport. I am convinced that the rehabilitation was successful for me. I had advantages: my age is 55 years old, my qualifications, which helped me realize and understand the sad events. I trained constantly to make it easier to adapt to life. I am an open, honest person and have never lost heart. I was interested in everything that would help me survive, and in order to avoid any awkwardness or misunderstanding, I chatted openly with the elderly nannies. I also had a lot of support from my family and friends.”
Robin Paul, T12
Your intestines
Immediately after the injury, your intestines will be sluggish, atonic, i.e. his muscles will not contract, although he will continue to function, eat food and absorb nutrients. Later, depending on the level of injury, you may develop or spastic intestines reflex type , or your intestines will remain sluggish, atonic .
Spastic bowel
If you have an injury above T12, your bowels will likely move reflexively. When the spinal cord is damaged, the feeling of filling the rectum does not reach the brain, but it does reach the spinal cord. As the rectum fills and stretches, it puts pressure on the nerve endings of the intestines. This causes a sensory signal that is sent from the intestines through sacral nerves of the sacral plexus to the intestinal muscles. At this moment, its contraction occurs.
Sluggish bowel
With injury at the L1 level and below, the bowel will most likely not have reflex activity. This occurs because the spinal cord ends at this level and signals from the nerve endings in the rectum cannot travel along the sacral plexus nerves to the spinal cord. The intestinal muscles will not contract, and the annular muscle of the anus (anal sphincter) will remain relaxed.

You will have to learn to regulate your food intake and bowel movements differently. A proper regulatory program will help you regain bowel control and maintain health. This is described in more detail below in the chapter.
Your bladder
Urination is one of the most important body care activities. “Going to take a leak” is the final stage of a simple but important process, because the elimination system is constantly working and monitors the amount of fluid in the body and its waste products. It serves as a kind of filter that cleanses the blood and facilitates blood flow.
Damage to the spinal cord somehow affects the ability to urinate normally. Even the most minor disturbances will cause a break in the “control chain” in this system, however, there are a number of methods that allow you to establish control over the functioning of the bladder. Learning the correct techniques for this adjustment will allow you, both now and in the future, to avoid infections, kidney and bladder stones, and other complications. This is described in more detail below in a special chapter. Bladder.
“Do not allow thoughts into your mind that you cannot do something. Try different ways to accomplish a particular task and after hundreds of unsuccessful attempts, you will find a way that will eventually work. The first time I spent half an hour fastening the zippers on my jeans, the second time it took 20 minutes, and now it only takes 25 seconds. At first everything was difficult for me, but now I can do almost everything.”
Tim Johnson, S6/7
Skin and sensitivity
Pairs of peripheral nerves that branch from the spinal cord carry sensory messages to the brain from specific areas of the body. When talking about sensitivity, such areas of the skin are called dermatomes . They are outlined very clearly and help doctors accurately determine which part of the spinal cord is damaged. The relative positions of the vertebrae, peripheral nerves and dermatomes can be understood from the corresponding figures.
Each pair of peripheral nerves also sends motor signals to muscle groups located near the corresponding dermatome. When talking about motor messages, these same areas are called myotomes .
If you have installed full break , this means that at the level of your injury there is a complete blockage of nerve connections. If the break is incomplete , then the blockade is only partial, and below the level of injury, sensitivity and movement are partially or completely preserved.
By testing the function of various muscles and skin sensitivity, doctors usually determine the level of your injury.

If you have no sensation below the level of injury, the brain does not receive signals from these areas of the skin about whether they have enough blood supply, whether they are overheated or cold, or whether they have cuts, punctures or abrasions.
If you are in a monotonous sitting or lying position for a long time, small areas of the body experience compression, which compresses very thin blood vessels that supply oxygen and food to the tissues. Most often this occurs over bony prominences, i.e. where the bones come closest to the surface of the skin. If such starvation from lack of “fuel” continues for a long time, tissues will begin to die and develop bedsore .
Damage to the spinal cord means that you must consciously make it a rule to carefully care for your skin. Since you don't respond to possible damage skin, now you must anticipate them in advance and prevent their occurrence. To contain skin at your best and stay away from the hospital, you'll have to learn the skills relieve compression by pushing the body away from the bed or stroller, turning or any other change in body position. Read the chapter carefully Skin.
Recovery card
Remember: This is just a sample! Start getting up only after complete healing. It takes at least a week to treat a sore of the second stage of development. Do not start the task the next day if your skin condition worsens or the improvement stops.
|
Days |
Recovery |
State |
|
Initial rise for half an hour. Return to bed and examine the skin area immediately and after 2 hours |
||
|
Half an hour in the morning. 4 hours of lying in a place other than the area of the bedsore. Half an hour in the afternoon. |
||
|
1 hour in the morning. 4 hours of lying in a place other than the area of the bedsore. 1 hour in the afternoon |
||
|
An hour and a half in the morning. 4 hours lying down. One and a half hours in the afternoon |
||
|
2 o'clock in the morning. 4 hours lying down. 2 hours in the afternoon |
||
|
Two and a half hours in the morning. 3 hours lying down. Two and a half hours in the afternoon |
||
|
3 o'clock in the morning. 3 hours lying down. 3 hours in the afternoon. |
||
|
3 and a half hours in the morning. 2 hours lying down. 3 and a half hours in the afternoon |
||
|
4 o'clock in the morning. Lying down for two hours. 4 hours in the afternoon |
||
|
Sitting all day with a two-hour break during the day. Next, reduce the break to half an hour. |
Hope for recovery and healing
Recovery
As we have already said, the outcome of your injury is initially masked by spinal shock. You may be tempted to not participate in rehabilitation, hoping that once the injury subsides, all body functions will recover on their own.
It is true that with the same level of damage, especially with incomplete break spinal cord, final results may be different. But the hope of restoring lost functions should not keep you from participating in rehabilitation. If you work hard now, it will be easier for you to use the restored functions in the future. Plus, you'll get out of the hospital sooner!
Complete cure
You will, of course, want to know what the likelihood of your complete recovery is. A spinal cord lesion is not a disease in itself, even if it is sometimes caused by a disease, and therefore the word “cure” cannot be applied to it. As with other injuries, doctors treat the symptoms and consequences of the injury as successfully as modern medicine can. Spinal cord injury is one of the most challenging physical injuries. At the time this book was written (2004 - L.I.), there were about 200 different international scientific programs studying all aspects of spinal cord injury and restoration of spinal cord functions (its regeneration ). There are many encouraging discoveries, but so far none of these studies can successfully restore lost function after complete severing of the spinal cord.
It is reasonable to assume that if ongoing advances in medical technology ever allow surgeons to restore the function of a damaged spinal cord, it is likely that these procedures will initially only be applied to “fresh” injuries. This is due to the fact that after an injury, the body itself additionally destroys the site of injury. It seems that the first successes on this path will be associated precisely with the prevention of this “corrosion” of the affected area, which occurs in the first two days after the injury. As for long-standing injuries, their recovery will be much more difficult than fresh injuries.
After injury, those affected nerve cells lose calcium ions and other substances that destroy the protective myelin coating of nerves and other cell membranes.
This chain reaction damages nerve cells near the site of injury that might otherwise be repaired. This damage appears to be exacerbated by a lack of oxygen. Many studies are aimed specifically at preventing these secondary injuries in order to reduce the overall effects of injury. If you would like to learn more about this, you can consult the many publications and websites that provide research on spinal cord injury.
Keep in mind that no two spinal cord injuries are alike. Depending on the cause of the injury, some spinal cord fibers may remain intact. The following terms are used to classify the type and extent of damage.
We do not intend to deprive you of hope for a final cure, but at the same time we want to inspire you to immediately do everything in your power for an active and joyful life! If you sit and wait for your “maybe”, then everything will end in deep disappointment, and you will miss the opportunities that exist now.
Important Concepts
Spinal cord lesion
Any injury to the spinal cord is called defeat. If it is caused by mechanical trauma, it is called traumatic injury.
Damage level
Spinal cord injuries are differentiated in medicine by the level of damage to the spinal cord.
Damage level bone part spine described by its section and vertebral number. (For example: cervical spine, 6th and 7th vertebrae = C6/7).
Neurological level indicates which nerves are affected; this is followed by an indication of complete or incomplete defeat.
Complete defeat
A complete lesion means that there is a complete blockage of nerve conduction at the site of injury.
Incomplete defeat
An incomplete lesion means that there is only a partial blockage of nerve conduction and some (or all) movement and sensation remain intact below the level of injury. The extent to which they are preserved depends on how severely your spinal cord is damaged. There are 5 main types of incomplete lesions:
Central cortical syndrome
Damage to the central part of the spinal cord usually occurs due to trauma to the cervical spine. You experience complete immobility of your arms, although you still have some movement in your legs. Sensation on the hands is usually located randomly. The bladder and intestines usually remain partially intact, and recovery is possible starting from the lower extremities and moving upward.
Posterior cortical syndrome
If the posterior part of the spinal cord is damaged, muscle strength and pain temperature sensitivity may be preserved, but difficulty coordinating movements may occur. This type is very rare.
Brown-Segard syndrome
This type occurs with lateral damage to the spinal cord. On the affected side of the body, muscle strength may be weakened or absent, and the sense of pressure and body position are impaired. On the opposite side, there is a loss or weakening of pain and temperature sensitivity, but movements, sensations of pressure and body position, as a rule, remain.
Cauda equina syndrome
The cauda equina is a bundle of nerves that radiate from the lower part of the spinal cord. Trauma to the cauda equina can cause patchy loss of muscle strength and sensation in the lower extremities. The intestines and bladder are usually seriously affected. If the nerve roots of the cauda equina are not completely crushed, functional recovery may occur after 12-18 months.
Paralysis
The word paralysis generally refers to the inability to freely move or feel certain parts of the body.
Paraplegia
The term paraplegia describes paralysis from the level below the cervical vertebrae ( below T1). Persons with paraplegia ( paraplegics, “spinal sufferers”) suffer from partial or complete paralysis of arms or legs.
Anterior cortical syndrome
When the anterior part of the spinal cord is damaged below the level of injury, there is usually complete or partial loss of movement, as well as pain, temperature and tactile (tactile) sensation. You may still have deep pressure sensation and positional awareness.
Tetraplegia (quardiplegia)
Persons with lesions of the cervical spine, “collars,” suffer from partial or complete paralysis of the arms and legs. Abroad they are called tetraplegics (tetra - four, Greek - L.I.), and in America quadriplegics (quad- four, lat.- L.), since all four limbs are affected.
Neurological damage
Any injury in which the spinal cord is damaged is called by doctors " neurological damage " A back injury in which the spinal cord is not affected is called a “non-neurological injury.” This means that the nervous system is not damaged and remains normal. Most patients with such an injury will be seen not in the spinal (neurosurgery) hospital units, but by orthopedic specialists.
“When I was in rehabilitation, I learned a lot from other spinal and cervical surgeons who came into the department for re-examination.
They provided me with a lot of useful advice and information. It seems to me that I paid more attention to them also because they were wheelchair users. I probably had more confidence in them."
Keith Jarvie, C4/5
“I remember the first time I got into the car. I was able to go on my own, which means I became more independent. But you still had to climb in and out on your own! At first I I made sure there was no one nearby. I was out of town with friends and decided to return home alone. They saw me getting into the car and offered to help, but I had to do it myself. Getting into the car is not difficult, but getting out is much more difficult. So I went home and spent 15-20 minutes getting out of the car. Now it takes 1 minute!
Tim Johnson, S6/7
“I remember well how we arrived from the airport to the spinal ward after what seemed like a long and slow ambulance ride. All I could see along the way were the tops of the street lamps. My wife was with me, and we waited in the corridor for a very long time, completely unaware of what was happening and what we should do. The wife is usually not very emotional, but then she was in the early stages of pregnancy, which we, however, did not yet know about, and therefore she was extremely excited and ready to cry. It was a bad start, but then gradually everything settled down and, to the benefit of the matter, it turned out to be friendly concern on her part.”
Ian Popeye, T5
Candidate of Medical Sciences Pavel Musienko, Institute of Physiology named after. I. P. Pavlova RAS (St. Petersburg).
The spinal cord can be “taught” to serve motor functions, even when its connection with the brain is disrupted as a result of injury, and moreover, it can be forced to form new connections “bypassing” the injury. This requires electrochemical neuroprostheses, stimulation and training.
Through the introduction of chemicals, they act on neuronal receptors, causing certain effects of excitation or inhibition of spinal cord neurons below the level of damage.
In case of paralysis, it is possible to stimulate the sensory fibers of the spinal cord and through them the spinal neurons (A) with an electric current. Thanks to electrical stimulation (ES), an animal with spinal cord injury can walk (B).
Motor skills in paralysis can be trained using a specially designed robotic system. The robot, if necessary, supports and controls the animal’s movements in three directions (x, y, z) and around vertical axis (φ
Multisystem neurorehabilitation (specific training + electrochemical stimulation) restores voluntary control of movements due to the formation of new interneuron connections in the spinal cord and brain stem.
For electrical stimulation of several segments of the spinal cord and multicomponent pharmacological stimulation of specific neuronal receptors on spinal networks, special neuroprostheses can be created - a set of electrodes and chemotrodes.
Spinal cord injuries are rarely accompanied by a complete anatomical interruption. Nerve fibers that remain intact can promote functional recovery.
The traditional neurophysiological picture of motor control assigned to the spinal cord the functions of a channel through which nerve impulses travel, connecting the brain with the body, and primitive reflex control. However, data accumulated by neurophysiologists recently force us to reconsider this modest role. New research technologies have made it possible to discover in the spinal cord numerous networks of its “own” neurons, specialized in performing complex motor tasks, such as coordinated walking, maintaining balance, and controlling speed and direction during movement.
Could these spinal cord neural systems be used to restore motor function in people paralyzed by spinal injury?
With a spinal cord injury, the patient loses motor functions because the connection between the brain and the body is disrupted or completely broken: the signal does not pass through, and motor neurons are not activated below the site of injury. Thus, an injury to the cervical spinal cord can lead to paralysis and loss of function of the arms and legs, so-called tetraplegia, and an injury to the thoracic region can lead to paraplegia, immobilization of only the lower extremities: as if units of a certain army, functional and combat-ready in themselves, turned out to be cut off from headquarters and stopped receiving commands.
But the main evil of spinal injury is that any stable connections connecting neurons into stable functional networks degrade if they are not activated again and again. Those who haven't ridden a bike or played the piano for a long time are familiar with this phenomenon: many motor skills are lost if they are not used. Similarly, in the absence of activating signals and training, the movement-specific neural networks of the spinal cord begin to disintegrate over time. The changes become irreversible: the network “forgets how” to move.
Can this be prevented? The answer given by modern neurophysiology is encouraging.
Neurons interact with each other sequentially, along a chain, producing chemicals - mediators of various types. At the same time, the majority of neurons are concentrated in the brain, using fairly well-studied monoaminergic mediators as a signal “language”: serotonin, norepinephrine, dopamine.
On the neural networks of even a damaged spinal cord, there are receptors that can perceive this signal. Therefore, one can try to activate the spinal networks with the help of appropriate monoaminergic drugs, introducing them into the nervous tissue of the spinal cord from the outside.
This circumstance formed the basis for experiments on chemical stimulation.
In 2008, together with a group of researchers from the University of Zurich (Switzerland), we tried to activate the spinal neural networks responsible for movement by “placing” substances corresponding to monoaminergic mediators on the intact receptors of spinal neurons. These drugs were supposed to serve as a source of a signal that activated the neural networks of the spinal cord and prevented their degradation. The result of the experiment was positive; moreover, optimal combinations of monoaminergic drugs were found to improve walking function and balance. The work was published in 2011 in the journal Neuroscience.
The spinal cord is distinguished by high systemic neuronal plasticity: its neural networks are able to gradually “remember” the tasks that they have to perform regularly. Regular exposure to certain sensory and motor pathways during motor training improves the functioning of these neural pathways and restores the ability to perform the trained functions.
But if the neural networks of the spinal cord can be trained, is it not possible to “teach” them something - for example, using stimulation of the damaged spinal cord and motor training to achieve such a functional restructuring of its neural networks that would control motor activity independently with greater or lesser success? , in isolation from the “main headquarters” - the brain?
To answer this question, we tried combining chemical neurostimulation with electrical one. Back in 2007, joint experiments by Russian and American neurophysiologists showed that if electrodes are placed on the surface of the spinal cord of a rat, the electric field around the active electrode can excite conducting spinal structures. Since very small currents were used in the experiment, the most excitable tissues near the electrode were activated first: the thick conducting fibers of the dorsal spinal roots, which transmit sensory information from the receptors of the tissues of the limbs to the neurons of the spinal cord. Such electrical stimulation made it possible to activate motor functions in spinal animals.
The combination of electrical stimulation, chemical stimulation and motor training gave excellent results. With a complete severance of the connections between the spinal cord and the brain, the “sleeping” spinal neural networks could be transformed into highly functionally active ones. Paralyzed animals were administered neuropharmacological drugs, their spinal cord was stimulated in two segments, and gait function was continuously trained. As a result, after a few weeks the animals showed movements close to normal and were able to adapt to changes in the speed and direction of movement.
In the first experiments, the researchers trained animals using a treadmill and a biomechanical system that helped the animal balance its body, but did not allow it to move forward. Recently, in 2012, the journals Science and Nature Medicine published the results of joint research by the University of Zurich and the Institute of Physiology. I.P. Pavlova RAS, in which we applied a robotic approach.
A special robot gives the rat the opportunity to move freely, if necessary supporting and controlling its movements in three directions (x, y, z). Moreover, the force of influence along various axes can vary depending on the experimental task and the animal’s own motor abilities. The robotic installation uses soft elastic drives and spirals that eliminate the inertial influence of force on a living object. This makes it possible to apply the installation in behavioral experiments. The robot was tested on an experimental model of a paralyzed rat with damage to the opposite halves of the spinal cord at the level of different spinal segments. The connection between the brain and spinal cord was completely interrupted, but there was still the possibility of new nerve fibers sprouting between the left and right sides spinal cord. (This pattern has similarities to spinal cord injuries in humans, which are often anatomically deficient.) The combination of training in a robotic system with multi-component chemical and electrical stimulation of the spinal cord allowed such animals to walk forward in a straight line, step over obstacles, and even climb stairs. The rats developed new interneuronal connections in the area of spinal cord damage and regained voluntary control of movements.
Thus was born the idea of electrochemical neuroprostheses for implantation into the spinal cord and control of spinal networks. Through special channels of the implant, drugs can be administered that act on the corresponding receptors and imitate the modulating nerve signal interrupted after injury. The electrode array stimulates the sensory inputs of different segments and through them activates separate populations of neurons to thereby cause specific movements.
Standard clinical approach Treatment of patients with severe spinal injuries is aimed at preventing further secondary damage to the nervous system, somatic complications of paralysis, providing psychological assistance to paralyzed patients and training them in the use of remaining functions. Restorative therapy for lost motor skills in severe spinal cord injuries is not only possible, but also necessary.
Experimental work on a chemical neuroprosthesis has not yet moved beyond laboratory studies on animals, but in 2011, the authoritative medical journal The Lancet provided a vivid illustration of what stimulation therapy can do in humans. The journal published the results of clinical experimental work using electrical stimulation of the spinal cord. Neurophysiologists and doctors from the USA and Russia showed that regular training of certain motor skills in combination with epidural stimulation of the spinal cord restored motor abilities in a patient with complete motor paraplegia, that is, complete loss of control over movement. The treatment improved the functions of standing and maintaining body weight, elements of locomotor activity and partial voluntary control of movements during stimulation.
As a result of training and stimulation, it was possible not only to activate neural networks below the level of damage, but also to a certain extent to restore the connection between the brain and spinal motor centers - the already mentioned neuroplasticity of the spinal cord made possible education new neural connections that “bypass” the site of injury.
Experimental and clinical researches show the high effectiveness of spinal cord stimulation and training after severe vertebrospinal injury. Although successful results have already been obtained with spinal cord stimulation in patients with severe paralysis, the bulk of the research work remains to be done. In addition, spinal implants for electrochemical stimulation must be developed and optimal algorithms for their use must be found. The world's leading laboratories are currently focusing their efforts on all this. Hundreds of independent and interlaboratory research projects are dedicated to achieving these goals. We can only hope that as a result of the joint efforts of world scientific centers, generally accepted clinical standards will include more effective methods treatment of paralyzed patients.
To control the functioning of the entire organism or each individual organ or motor apparatus, the spinal cord pathways are required. Their main task is to deliver impulses sent by the human “computer” to the body and limbs. Any failure in the process of sending or receiving impulses of a reflex or sympathetic nature is fraught with serious pathologies of health and all life activity.
What are the pathways in the spinal cord and brain?
The pathways of the brain and spinal cord act as a complex of neural structures. During their work, impulses are sent to specific areas of the gray matter. Essentially, impulses are signals that prompt the body to act upon the call of the brain. Several groups of different according to functional features, are the conductive tracts of the spinal cord. These include:
- projection nerve endings;
- associative paths;
- commissural connecting roots.
In addition, the performance of spinal conductors necessitates the following classification, according to which they can be:
- motor;
- sensory.
Sensory perception and motor activity of a person
The sensory or sensitive pathways of the spinal cord and brain serve as an indispensable element of contact between these two complex systems in the body. They send an impulsive message to every organ, muscle fiber, arms and legs. The instantaneous sending of an impulse signal is a fundamental moment in the implementation by a person of coordinated coordinated body movements, performed without any conscious effort. Impulses sent by the brain can be recognized by nerve fibers through the sense of touch, pain, body temperature, and joint and muscle motility.
The motor pathways of the spinal cord determine the quality of a person’s reflex response. By ensuring the sending of impulse signals from the head to the reflex endings of the ridge and the muscular system, they endow a person with the ability to self-control motor skills - coordination. Also, these pathways are responsible for transmitting stimulating impulses towards the visual and auditory organs.
Where are the pathways located?
Having become familiar with the anatomical distinctive features of the spinal cord, it is necessary to understand where the very conductive tracts of the spinal cord are located, because this term implies a lot of nerve matter and fibers. They are located in specific vital necessary substances: gray and white. Connecting the spinal horns and the cortex of the left and right hemispheres, the pathways through neural communication provide contact between these two sections.
Functions of the most important conductors human organs consist in the implementation of intended tasks with the help of specific departments. In particular, the spinal cord pathways are located within the upper vertebrae and head; this can be described in more detail as follows:
- Associative connections are a kind of “bridges” that connect the areas between the cerebral cortex and the nuclei of the spinal substance. Their structure contains fibers of various sizes. Relatively short ones do not extend beyond the hemisphere or its cerebral lobe. Longer neurons transmit impulses that travel over some distance to the gray matter.
- The commissural tract is a body that has a callosal structure and performs the task of connecting the newly formed sections in the head and spinal cord. The fibers from the main lobe spread out in a radial manner and are located in the white spinal substantia.
- Projection nerve fibers are located directly in the spinal cord. Their performance makes it possible for impulses to arise in the hemispheres in a short time and establish communication with internal organs. The division into ascending and descending pathways of the spinal cord concerns specifically fibers of this type.
System of ascending and descending conductors
The ascending pathways of the spinal cord fulfill the human need for vision, hearing, motor functions and their contact with important systems body. The receptors for these connections are located in the space between the hypothalamus and the first segments of the spinal column. The ascending tracts of the spinal cord are capable of receiving and sending further impulses coming from the surface of the upper layers of the epidermis and mucous membranes, life support organs.

In turn, the descending pathways of the spinal cord include the following elements in their system:
- The neuron is pyramidal (originates in the cerebral cortex, then rushes down, bypassing the brain stem; each of its bundles is located on the spinal horns).
- The neuron is central (it is a motor neuron, connecting the anterior horns and the cerebral cortex with reflex roots; along with the axons, the chain also includes elements of the peripheral nervous system).
- Spinocerebellar fibers (conductors of the lower extremities and the spinal cord, including the sphenoid and thin ligaments).
It is quite difficult for an ordinary person who does not specialize in neurosurgery to understand the system represented by the complex pathways of the spinal cord. The anatomy of this department is truly an intricate structure consisting of neural impulse transmissions. But it is thanks to it that the human body exists as a single whole. Due to the double direction along which the spinal cord conductive pathways operate, instant transmission of impulses is ensured, which carry information from the controlled organs.
Conductors of deep sensory
The structure of the nerve ligaments, acting in the ascending direction, is multi-component. These spinal cord pathways are formed by several elements:
- Burdach's bundle and Gaulle's bundle (represent pathways of deep sensitivity located on the posterior side of the spinal column);
- spinothalamic bundle (located on the side of the spinal column);
- Govers' bundle and Flexig's bundle (cerebellar tracts located on the sides of the column).
Inside the intervertebral nodes there is a deep degree of sensitivity. The processes, localized in peripheral areas, end in the most suitable muscle tissues, tendons, osteochondral fibers and their receptors.

In turn, the central processes of the cells, located behind, are directed towards the spinal cord. Conducting deep sensitivity, the posterior nerve roots do not go deep into the gray matter, forming only the posterior spinal columns.
Where such fibers enter the spinal cord, they are divided into short and long. Next, the pathways of the spinal cord and brain are sent to the hemispheres, where their radical redistribution occurs. The main part of them remains in the areas of the anterior and posterior central gyri, as well as in the region of the crown.
It follows that these pathways conduct sensitivity, thanks to which a person can feel how his muscular-articular apparatus works, feel any vibration movement or tactile touch. The Gaulle bundle, located right in the center of the spinal cord, distributes sensation from the lower torso. Burdach's bundle is located higher and serves as a conductor of sensitivity of the upper extremities and the corresponding part of the body.
How to find out about the degree of sensory?
The degree of deep sensitivity can be determined using several simple tests. To perform them, the patient's eyes are closed. Its task is to determine the specific direction in which the doctor or researcher makes passive movements in the joints of the fingers, arms or legs. It is also advisable to describe in detail the posture of the body or the position taken by its limbs.
Using a tuning fork, the spinal cord pathways can be examined for vibration sensitivity. The functions of this device will help to accurately determine the time during which the patient clearly feels vibration. To do this, take the device and press it to make a sound. At this point, it is necessary to expose to any bony prominence on the body. In the case when such sensitivity disappears earlier than in other cases, it can be assumed that the posterior columns are affected.
The test for the sense of localization involves the patient, with his eyes closed, accurately pointing to the place where the researcher touched him a few seconds before. The indicator is considered satisfactory if the patient makes an error within one centimeter.
Sensory sensitivity of the skin
The structure of the spinal cord pathways makes it possible to determine the degree of skin sensitivity at the peripheral level. The fact is that the nerve processes of the protoneuron are involved in skin receptors. The processes located centrally as part of the posterior processes rush directly to the spinal cord, as a result of which Lisauer’s area is formed there.

Just like the path of deep sensitivity, the cutaneous one consists of several sequentially united nerve cells. Compared to the spinothalamic bundle of nerve fibers, information impulses transmitted from the lower extremities or lower torso are slightly above and in the middle.
Skin sensitivity varies according to criteria based on the nature of the irritant. It happens:
- temperature;
- thermal;
- painful;
- tactile.
In this case, the latter type of skin sensitivity, as a rule, is transmitted by conductors of deep sensitivity.
How to find out about the pain threshold and temperature differences?
To determine the level of pain, doctors use the pricking method. In the most unexpected places for the patient, the doctor applies several light injections with a pin. The patient's eyes should be closed, because He shouldn't see what's happening.
The temperature sensitivity threshold is easy to determine. In a normal state, a person experiences different sensations at temperatures, the difference of which was about 1-2°. To identify a pathological defect in the form of impaired skin sensitivity, doctors use a special device - a thermoesthesiometer. If it is not there, you can test for warm and hot water.
Pathologies associated with disruption of conduction pathways
In the ascending direction, the spinal cord pathways are formed in a position due to which a person can feel tactile touch. For the study, you need to take something soft, tender and, in a rhythmic manner, conduct a subtle examination to identify the degree of sensitivity, as well as check the reaction of hairs, bristles, etc.

Disorders caused by skin sensitivity are currently considered to be:
- Anesthesia is the complete loss of skin sensation in a specific superficial area of the body. When pain sensitivity is impaired, analgesia occurs, and when temperature sensitivity occurs, thermaneesthesia occurs.
- Hyperesthesia is the opposite of anesthesia, a phenomenon that occurs when the excitation threshold decreases; when it increases, hypalgesia appears.
- Misperception irritating factors(for example, the patient confuses cold and warm) is called dysesthesia.
- Paresthesia is a disorder, the manifestations of which can be huge, ranging from crawling goose bumps, the feeling of an electric shock and its passage through the entire body.
- Hyperpathy has the most pronounced severity. It is also characterized by damage to the visual thalamus, an increase in the threshold of excitability, the inability to locally identify the stimulus, a severe psycho-emotional coloring of everything that happens, and an overly sharp motor reaction.
Features of the structure of descending conductors
The descending pathways of the brain and spinal cord include several ligaments, including:
- pyramidal;
- rubrospinal;
- vestibulo-spinal;
- reticulospinal;
- rear longitudinal.
All of the above elements are motor pathways of the spinal cord, which are components of the nerve cords in the descending direction.
The so-called begins from huge cells of the same name located in the upper layer of the cerebral hemisphere, mainly in the area of the central gyrus. The conducting path of the anterior cord of the spinal cord is also located here - this important element system is directed downward and passes through several sections of the posterior femoral capsule. At the point of intersection of the medulla oblongata and the spinal cord, an incomplete decussation can be found, forming a straight pyramidal fasciculus.
In the tegmentum of the midbrain there is a conducting rubro-spinal tract. It starts from red kernels. Upon exiting, its fibers intersect and pass into the spinal cord through the varoli and medulla oblongata. The rubrospinal tract allows impulses to be transmitted from the cerebellum and subcortical ganglia.
The spinal cord pathways begin in Deiters' nucleus. Located in the brain stem, the vestibulospinal tract continues in the spinal tract and ends in its anterior horns. The passage of impulses from the vestibular apparatus to the peripheral system depends on this conductor.
In the cells of the reticular formation of the hindbrain, the reticulospinal tract begins, which in the white matter of the spinal cord is scattered in separate bundles mainly from the side and in front. In fact, this is the main connecting element between the reflex brain center and the musculoskeletal system.
The posterior longitudinal ligament is also involved in connecting motor structures to the brain stem. The work of the oculomotor nuclei and the vestibular apparatus as a whole depends on it. The posterior longitudinal fasciculus is located in the cervical spine.
Consequences of spinal cord diseases
Thus, the spinal cord pathways are vital connecting elements that provide a person with the ability to move and feel. The neurophysiology of these pathways is associated with the structural features of the spine. It is known that the structure of the spinal cord, surrounded by muscle fibers, has a cylindrical shape. Inside the spinal substances brain stem associative and motor reflex pathways control the functionality of all body systems.

If spinal cord disease, mechanical damage, or developmental defects occur, conduction between the two main centers can be significantly reduced. Disorders of the pathways threaten a person with a complete cessation of motor activity and loss of sensory perception.
The main reason for the lack of impulse conduction is the death of nerve endings. The most complex degree of conduction disturbance between the brain and spinal cord is paralysis and lack of sensation in the limbs. Then problems may occur in the functioning of internal organs connected to the brain by damaged neural ligaments. For example, disorders in the lower part of the spinal trunk result in uncontrollable urination and defecation processes.
Are diseases of the spinal cord and pathways treated?
As soon as degenerative changes appear, they almost immediately affect the conductive activity of the spinal cord. Suppression of reflexes leads to pronounced pathological changes caused by the death of neuron fibers. It is impossible to completely restore damaged areas of conductivity. The disease occurs rapidly and progresses at lightning speed, so avoid gross violations conductivity is possible only if you start in a timely manner drug treatment. The sooner this is done, the greater the chances of stopping pathological development.
Non-conductivity of the spinal cord pathways requires treatment, priority which will stop the processes of death of nerve endings. This can only be achieved if the factors that influenced the occurrence of the disease are suppressed. Only after this can you begin therapy with the goal of maximizing possible restoration sensitivity and motor functions.
Treatment with medications is aimed at stopping the process of death of brain cells. Their task is also to restore impaired blood supply to the damaged area of the spinal cord. During treatment, doctors take into account age characteristics, nature and severity of damage and progression of the disease. In pathway therapy, it is important to maintain constant stimulation of nerve fibers using electrical impulses. This will help maintain satisfactory muscle tone.

Surgical intervention is carried out to restore the conductivity of the spinal cord, so it is carried out in two directions:
- Suppressing the causes of paralysis of the activity of neural connections.
- Stimulation of the spinal trunk for the rapid acquisition of lost functions.
The operation must be preceded by a complete medical examination of the entire body. This will allow us to determine the localization of the processes of degeneration of nerve fibers. In the case of severe spinal injuries, the causes of compression must first be eliminated.
22. The cerebellum, its connections with the spinal cord and brain. Symptoms of the lesion
The cerebellum is also connected by special pathways to the cerebral cortex and spinal cord. The cerebellum performs a complex reflex function of balance. Along the spinocerebellar tract, through the lower peduncles, impulses that arise in connection with changes in the position of joints, muscles and tendons, as well as a number of other impulses from the posterior columns of the spinal cord, are sent to the cerebellum.
Pathways in the superior cerebellar peduncles depart from the dentate nucleus of the cerebellum, which carry impulses to the red nuclei of the midbrain. The so-called Monaco bundle departs from the red nuclei, carrying impulses to the spinal cord. In this way, a complex balance system is implemented, where the cerebellum plays the role of a regulatory organ that makes corrections to every voluntary movement carried out by a certain group of muscles. The mechanism of these amendments is that the cerebellum, including antagonist muscle groups, simultaneously removes the inertia that is inherent in each motor act. Due to damage to the fibers of the cerebellar tract, movement coordination disorders occur. When the posterior columns are damaged, deep sensitivity is impaired - the sense of position of the organs of movement, localization, two-dimensional spatial sense. In this regard, the gait is also disrupted, which becomes uncertain, movements are sweeping, imprecise
23. Extrapyramidal system
Cerebellar lesion syndrome
Cerebellar lesion syndrome is expressed in disturbances of balance, coordination of movements and muscle tone.
Balance disorders are manifested by static ataxia. If statics are disturbed, the patient in the Romberg groove deviates towards the affected cerebellar hemisphere. IN severe cases the static disorder is so pronounced that the patient cannot sit or stand even with his legs spread wide apart. Adiadochokinesis is also detected - impaired alternation of opposite movements. Adiadochokinesis is detected when the patient tries to quickly alternately supinate and pronate the hand, resulting in awkward, imprecise movements.
Pallidal system lesion syndrome. The symptom complex of damage to the pallidal system is called parkinsonism. The main symptoms of parkinsonism are impaired motor activity and muscle hypertension. The patient's movements become poor, inexpressive (oligokinesia) and slow (bradykenesia). With parkinsonism, tremor is noted in the fingers and (sometimes) in the lower jaw. Tremor occurs at rest and is characterized by rhythm, small amplitude and low frequency. Since the main symptoms of damage to the pallidal system are hypokinesia and muscle hypertension, this symptom complex is also called hypokinetic-hypertensive. Striatal system lesion syndrome. When the striatal part of the extrapyramidal system is damaged, a hyperkinetic-hypotonic symptom complex is noted. The main symptoms are muscle hypotonia and excessive involuntary movements - hyperkinesis. The latter arise involuntarily, disappear during sleep, and intensify with movement. When studying hyperkinesis, attention is paid to their shape, symmetry, side and localization of manifestation (in the upper, or proximal, parts of the extremities or in the lower - distal). Hyperkinesis has various forms of manifestation. Hyperkinesis is usually accompanied by muscle hypotonia. They are often observed in children; arise as a result organic lesions striatal part of the extrapyramidal system due to the lack of inhibitory influence of the striatum on the underlying motor centers. However, children often experience functional (neurotic) hyperkinesis, which is in the nature of obsessive movements. They occur after fright, overwork, past diseases, traumatic brain injuries and experiences that are traumatic to the child’s psyche.
24. Paralysis (paresis) of a peripheral, central, hysterical nature
Peripheral paralysis is characterized by the following main symptoms: absence of reflexes or their decrease (hyporeflexia, areflexia), decrease or absence of muscle tone (atony or hypotonia), muscle atrophy. In addition, changes in electrical excitability, called the degeneration reaction, develop in paralyzed muscles and affected nerves. In peripheral paralysis, atrophied mice may exhibit fibrillary twitches in the form of rapid contractions of individual muscle fibers or bundles of muscle fibers (fascicular twitches). They are observed in chronic progressive pathological processes in peripheral motor neuron cells.
Damage to the peripheral nerve leads to peripheral paralysis muscles innervated by this nerve.
In this case, sensory disturbances and autonomic disorders are also observed in the same area, since the peripheral nerve is mixed - motor and sensory fibers pass through it. An example of peripheral paralysis of the limbs is the paralysis that occurs with polio, an acute infectious disease of the nervous system. With polio, paralysis of the legs, arms, and respiratory muscles can develop. When the cervical and thoracic segments of the spinal cord are affected, peripheral paralysis of the diaphragm and intercostal muscles is observed, leading to respiratory failure. Damage to the upper thickening of the spinal cord leads to peripheral paralysis of the arms, and the lower (lumbar thickening) leads to paralysis of the legs.
Central paralysis occurs when the central motor neuron is damaged in any part of it (motor cortex cerebral hemispheres, brain stem, spinal cord). A break in the pyramidal tract removes the influence of the cerebral cortex on the segmental reflex apparatus of the spinal cord; his own apparatus is disinhibited. In this regard, all the main signs of central paralysis are, in one way or another, associated with increased excitability of the peripheral segmental apparatus.
The main signs of central paralysis are muscle hypertension, hyperreflexia, expansion of the zone of evoking reflexes, foot clonus and kneecaps, pathological reflexes, protective reflexes and pathological synkinesis. Lesion of the pyramidal tract in the lateral column of the spinal cord causes central paralysis of the muscles below the level of the lesion. If the lesion is localized in the upper cervical segments of the spinal cord, then central hemiplegia develops, and if in the thoracic spinal cord, then central leg plegia. Central paralysis of facial muscles; differs from peripheral paralysis observed with neuritis of the facial nerve or with crossed Millard-Gubler syndrome in that only the muscles are affected lower half faces. With central paralysis of the tongue muscles, tongue atrophy does not develop.
Symptoms and prophets of the development of other organs and systems. Sometimes the detection of pathology in NSG is an accidental finding. III. Systematics of B-scanning methods of the brain from the perspective of pediatric neuropathology and neurosurgery Depending on the sensors used, linear scanning or sectoral scanning is performed. Depending on the ultrasonic window used, there are...
Laryngospasm. The pain radiates to the ear and is provoked by eating and swallowing. The pain point is determined on the lateral surface of the neck, slightly above the thyroid cartilage. Giving help. Emergency care is similar to that provided to patients with neuralgia trigeminal nerve. Glossalgia. Clinic. Glossalgia is caused by damage to the peripheral somatic formations of the oral cavity, but most importantly...


Activity and sound-pronunciation aspects of speech. Such children have a quiet, poorly modulated voice with a nasal tint. Study of the cervical-tonic reflex in cerebral palsy with torticollis symptoms. Depending on the severity and prevalence, the following forms of cerebral palsy are distinguished: spastic diplegia, spastic hemiplegia, double hemiplegia, ...
U. M., Belova L. V. “Some issues of psychotherapy in dermatology” - “Bulletin of Dermatology and Venereology” 1982, 11, 62-66. 605. Mirzamukhamedov M. A., Suleymanov A. S., Pak S. T., Shamirzaeva M. Kh. “The effectiveness of hypnosis and acupuncture in some functional diseases in children” - “Medical Journal of Uzbekistan” 1987, 1, 52-54 . 606. Mirzoyan A. S. “Step-by-step psychotherapy of sexual...
The human spinal cord is the most important organ of the central nervous system, connecting all organs with the central nervous system and conducting reflexes. It is covered on top with three shells:
- hard, cobwebby and soft
Between the arachnoid and soft (vascular) membrane and in its central canal there is cerebrospinal fluid (liquor)
IN epidural space (the space between solid meninges and the surface of the spine) - vessels and adipose tissue
Structure and functions of the human spinal cord
What is the external structure of the spinal cord?
This is a long cord spinal canal, in the form of a cylindrical cord, approximately 45 mm long, about 1 cm wide, flatter in front and behind than on the sides. It has a conditional upper and lower bound. The superior one begins between the line of the foramen magnum and the first cervical vertebra: At this point the spinal cord connects to the brain through the intermedius oblongata. The lower one is at the level of 1-2 lumbar vertebrae, after which the cord takes on a conical shape and then “degenerates” into a thin spinal cord ( terminal) with a diameter of about 1 mm, which stretches to the second vertebra of the coccygeal region. The terminal filament consists of two parts - internal and external:
- internal - approximately 15 cm long, consists of nerve tissue, intertwined by the lumbar and sacral nerves and located in a sac of dura mater
- outer - about 8 cm, begins below the 2nd vertebra of the sacral region and stretches in the form of a connection of the hard, arachnoid and soft membranes to the 2nd coccygeal vertebra and fuses with the periosteum
The outer terminal filament, hanging down to the coccyx, with the nerve fibers intertwining it, is very similar in appearance to a horse’s tail. Therefore, pain and phenomena that occur when nerves are pinched below the 2nd sacral vertebra are often called cauda equina syndrome.
The spinal cord has thickenings in the cervical and lumbosacral regions. This finds its explanation in the presence large quantity exiting nerves in these places, going to the upper as well as to the lower extremities:
- Cervical thickening extends from the 3rd - 4th cervical vertebrae to the 2nd thoracic vertebrae, reaching a maximum in the 5th - 6th
- Lumbosacral - from the level of the 9th - 10th thoracic vertebrae to the 1st lumbar with a maximum in the 12th thoracic
Gray and white matter of the spinal cord
If you look at the structure of the spinal cord in cross section, then in the center you can see a gray area in the form of a butterfly spreading its wings. This is the gray matter of the spinal cord. It is surrounded on the outside by a white substance. Cellular structure gray and white matter differ from each other, as do their functions.

The gray matter of the spinal cord consists of motor and interneurons:
- motor neurons transmit motor reflexes
- intercalary - provide communication between the neurons themselves
White matter consists of so-called axons— nerve processes from which the fibers of the descending and ascending pathways are created.
The wings of the “butterfly” are narrower and form front horns gray matter, wider - rear. The anterior horns contain motor neurons, in the rear - insertion. Between the symmetrical lateral parts there is a transverse bridge of brain tissue, in the center of which there is a channel communicating top part with a cerebral ventricle and filled with cerebrospinal fluid. In some sections or even along its entire length in adults, the central canal may become overgrown.
Relative to this canal, to the left and right of it, the gray matter of the spinal cord looks like symmetrically shaped columns connected to each other by anterior and posterior commissures:
- the anterior and posterior columns correspond to the anterior and posterior horns in cross section
- lateral projections form a side pillar
The lateral projections are not present along their entire length, but only between the 8th cervical and 2nd lumbar segments. Therefore, the cross section in segments where there are no lateral protrusions has an oval or round shape.
The connection of symmetrical columns in the anterior and posterior parts forms two grooves on the surface of the brain: the anterior, deeper one, and the posterior. The anterior fissure ends in a septum adjacent to the posterior border of the gray matter.
Spinal nerves and segments
To the left and right of these central grooves are located respectively anterolateral And posterolateral grooves through which the anterior and posterior filaments emerge ( axons), forming nerve roots. The anterior root in its structure is motor neurons anterior horn. The posterior one, responsible for sensitivity, consists of interneurons posterior horn. Immediately at the exit from the medullary segment, both the anterior and posterior roots unite into one nerve or nerve ganglion ( ganglion). Since in total in each segment there are two anterior and two dorsal roots, in total they form two spinal nerve(one on each side). Now it is not difficult to calculate how many nerves the human spinal cord has.
To do this, let us consider its segmental structure. There are 31 segments in total:
- 8 - in the cervical region
- 12 - in the chest
- 5 - lumbar
- 5 - in the sacrum
- 1 - in the coccygeal
This means that the spinal cord has only 62 nerves - 31 on each side.
The sections and segments of the spinal cord and spine are not at the same level due to the difference in length (the spinal cord is shorter than the spine). This must be taken into account when comparing the brain segment and vertebral number when performing radiology and tomography: if at the beginning of the cervical spine this level corresponds to the vertebral number, and in its lower part lies on the vertebra above, then in the sacral and coccygeal sections this difference is already several vertebrae.
Two important functions of the spinal cord
The spinal cord performs two important functions − reflex And conductor. Each of its segments is associated with specific organs, ensuring their functionality. For example:
- Cervical and thoracic region - connects with the head, arms, organs chest, chest muscles
- Lumbar region - gastrointestinal tract, kidneys, muscular system of the trunk
- Sacral region - pelvic organs, legs
Reflex functions are simple reflexes inherent in nature. For example:
- pain reaction - pull your hand away if it hurts.
- knee reflex
Reflexes can be carried out without the participation of the brain
This is proven simple experiments on animals. Biologists conducted experiments with frogs, checking how they react to pain in the absence of a head: a reaction was noted to both weak and strong painful stimuli.
The conductor functions of the spinal cord consist of conducting an impulse along the ascending path to the brain, and from there along the descending path in the form of a return command to some organ
Thanks to this conductive connection, any mental action is carried out:
get up, go, take, throw, lift, run, cut, draw- and many others that a person, without noticing, does in his daily life at home and at work.
Such a unique connection between the central brain, spinal cord, the entire central nervous system and all organs of the body and its limbs remains, as before, the dream of robotics. Not a single robot, even the most modern one, is yet capable of performing even a thousandth of those various movements and actions that are subject to the control of a biological organism. As a rule, such robots are programmed for highly specialized activities and are mainly used in automatic conveyor production.
Functions of gray and white matter. To understand how these magnificent functions of the spinal cord are carried out, consider the structure of the gray and white matter of the brain at the cellular level.
The gray matter of the spinal cord in the anterior horns contains large nerve cells called efferent(motor) and are combined into five nuclei:
- central
- anterolateral
- posterolateral
- anteromedial and posteromedial
The sensory roots of small cells of the dorsal horns are specific cell processes from the sensory ganglia of the spinal cord. In the dorsal horns, the structure of the gray matter is heterogeneous. Most of the cells form their own nuclei (central and thoracic). The border zone of the white matter, located near the posterior horns, is adjacent to the spongy and gelatinous zones of the gray matter, the cell processes of which, together with the processes of small diffusely scattered cells of the posterior horns, form synapses (contacts) with the neurons of the anterior horns and between adjacent segments. These neurites are called anterior, lateral and posterior bundles of their own. Their connection with the brain is carried out using white matter pathways. Along the edge of the horns, these tufts form a white border.
The lateral horns of gray matter perform the following important functions:
- In the intermediate zone of gray matter (lateral horns) there are sympathetic cells vegetative nervous system, it is through them that communication with internal organs is carried out. The processes of these cells connect to the anterior roots
- Here it is formed spinocerebellar path:
At the level of the cervical and upper thoracic segments there is reticular zone - a bundle of a large number of nerves associated with zones of activation of the cerebral cortex and reflex activity.

The segmental activity of the gray matter of the brain, the posterior and anterior roots of the nerves, and the own bundles of white matter bordering the gray is called the reflex function of the spinal cord. The reflexes themselves are called unconditional, according to Academician Pavlov’s definition.
The conductive functions of white matter are carried out through three cords - its outer sections, limited by grooves:
- Anterior funiculus - the area between the anterior median and lateral grooves
- Posterior funiculus - between the posterior median and lateral grooves
- Lateral funiculus - between the anterolateral and posterolateral grooves
White matter axons form three conduction systems:
- short bundles called associative fibers that connect different segments of the spinal cord
- ascending sensitive (afferent) beams directed to parts of the brain
- descending motor (efferent) bundles directed from the brain to the neurons of the gray matter of the anterior horns
Ascending and descending conduction pathways. Let's look at some of the functions of the white matter cord pathways as an example:
Front ropes:
- Anterior pyramidal (corticospinal) tract- transmission of motor impulses from the cerebral cortex to the spinal cord (anterior horns)
- Spinothalamic anterior tract- transmission of tactile impulses affecting the surface of the skin (tactile sensitivity)
- Tectospinal tract- connecting the visual centers under the cerebral cortex with the nuclei of the anterior horns, creates a protective reflex caused by sound or visual stimuli
- Bundle of Held and Leventhal (vestibular tract)- white matter fibers connect the vestibular nuclei of eight pairs of cranial nerves with motor neurons of the anterior horns
- Longitudinal posterior beam— connecting the upper segments of the spinal cord with the brain stem, coordinates the work eye muscles with cervical, etc.
The ascending pathways of the lateral cords carry impulses of deep sensitivity (feelings of one’s body) along the corticospinal, spinothalamic and tegmental spinal tracts.
Descending tracts of the lateral funiculi:
- Lateral corticospinal (pyramidal)- transmits the impulse of movement from the cerebral cortex to the gray matter of the anterior horns
- Red nuclear spinal tract(located in front of the lateral pyramidal), the spinocerebellar posterior and spinothalamic lateral tracts are adjacent to it.
The red nucleus spinal tract carries out automatic control of movements and muscle tone on a subconscious level.

Different parts of the spinal cord have different proportions of gray and white brain matter. This is explained by the different number of ascending and descending paths. The lower spinal segments have more gray matter. As you move upward, it becomes less, and the white matter, on the contrary, increases, as new ascending pathways are added, and at the level of the upper cervical segments and the middle part of the chest there is the most white. But in the area of both the cervical and lumbar thickenings, gray matter predominates.
As you can see, the spinal cord has a very complex structure. The connection between nerve bundles and fibers is vulnerable, and serious injury or illness can disrupt this structure and lead to disruption of the conduction pathways, which is why below the “break” point of conduction there can be complete paralysis and loss of sensitivity. Therefore, at the slightest dangerous sign, the spinal cord must be examined and treated promptly.
Spinal cord puncture
To diagnose infectious diseases (encephalitis, meningitis and other diseases), a spinal cord puncture (lumbar puncture) is used - inserting a needle into the spinal canal. It is carried out this way:
IN subarachnoid the space of the spinal cord at a level below the second lumbar vertebra is inserted with a needle and taken cerebrospinal fluid (cerebrospinal fluid).
This procedure is safe, since below the second vertebra in an adult there is no spinal cord, and therefore there is no threat of damage to it.
However, it requires special care so as not to introduce infection or epithelial cells under the membrane of the spinal cord.
Spinal cord puncture is performed not only for diagnosis, but also for treatment, in the following cases:
- injection of chemotherapy drugs or antibiotics under the lining of the brain
- for epidural anesthesia during operations
- for the treatment of hydrocephalus and reduction intracranial pressure(removal of excess cerebrospinal fluid)
Spinal cord puncture has the following contraindications:
- spinal canal stenosis
- displacement (dislocation) of the brain
- dehydration (dehydration)
Take care of this important organ, engage in basic prevention:
- Take antiviral medications during a viral meningitis epidemic
- Try not to have picnics in the forested area in May-early June (the period when the encephalitis tick is active)
