Ulcerative colitis disease symptoms. What is colitis? Acute stage therapy
2. Massive bleeding from the colon. Given the complication leads to anemia (decreased number of red blood cells and hemoglobin), as well as hypovolemic (reduced blood volume) shock.
3. Malignization (malignancy)– the appearance of a malignant tumor at the site of inflammation.
4. Secondary intestinal infections. Inflamed mucosa is a good environment for the development of intestinal infection. This complication significantly worsens the course of the disease. Diarrhea gets worse, stools 10-14 times a day, high fever, dehydration.
5. Purulent complications. For example, paraproctitis is an acute inflammation of the fatty tissue near the rectum. This purulent complication is treated surgically.
Treatment of UC

Effective treatment is only possible with a specialist doctor. Exacerbation of the disease can only be treated in a hospital.
Diet for UC
Diet principles1. All food must be boiled or baked.
2. Dishes should be consumed warm. Meal frequency – 5 times a day.
3. Last meal no later than 19.00.
4. The diet should be hypercaloric (high in calories) 2500-3000 calories per day. The exception is for obese patients.
5. The diet should be hyperprotein (high protein content)
6. Must contain increased amount vitamins and microelements
Prohibited Products
The products described below cause chemical and mechanical irritation of the colon mucosa. Irritation intensifies the inflammatory process. Also, some foods increase peristalsis (movement) of the large intestine, which worsens diarrhea.
- alcohol
- carbonated drinks
- dairy
- mushrooms
- fatty meats (duck, goose, pork)
- kiwi, plum, dried apricots
- any type of spice
- coffee, cocoa, strong tea, chocolate
- ketchup, mustard
- any peppered and highly salted dishes
- chips, popcorn, crackers
- raw vegetables
- nuts
- seeds
- legumes
- corn
Products to be consumed:
- fruits
- berries
- various slimy cereals
- boiled eggs
- low-fat meats (beef, chicken, rabbit)
- juice from tomatoes and oranges
- non-fatty fish
- liver
- cheese
- seafood
Drug treatment
 Drugs from the group of aminosalicylates are used. During an exacerbation, sulfasalazine is used orally 1 gram 3-4 times a day until remission occurs. In remission phase dose
Drugs from the group of aminosalicylates are used. During an exacerbation, sulfasalazine is used orally 1 gram 3-4 times a day until remission occurs. In remission phase dose 0.5-1 gram 2 times a day.
Mesalazine – 0.5-1 gram 3-4 times a day during exacerbation. In remission, 0.5 grams 2 times a day.
To treat ulcerative colitis in the area of the rectum and sigmoid colon, suppositories or enemas with salofalk or mesalazole are used.
Corticosteroids are used for severe forms of the disease. Prednisolone is prescribed orally at 40-60 milligrams per day, the duration of treatment is 2-4 weeks. After which the dose of the drug is reduced by 5 mg per week.
Recently, local corticosteroids have been used. Budesonide - 3 mg 3 times a day for 12 months, then 2 mg 3 times a day for another 6 weeks and then 1 mg 3 times a day for 6 weeks.
Immunosuppressants are also sometimes used. Cyclosporine A is used for acute and fulminant forms of the disease at a dose of 4 mg per kilogram of body weight intravenously. Or azathioprine orally at a dose of 2-3 mg per kilogram of body weight.
Symptomatic treatment. Different kinds anti-inflammatory drugs with pain relief, such as ibuprofen or paracetamol.
Vitamin therapy (vitamins B and C)
Prevention of UC
One of the most important preventive measures is diet. It is also important to have a preventive visit to a general practitioner and take blood and stool tests.
What traditional methods of treating UC exist?
In the treatment of UC, traditional medicine uses a number of food products of plant (and not only) origin, as well as decoctions and infusions prepared from these products.- Bananas
- Return
- Apples
- Congee
There is another effective recipe for the treatment of UC using rice:
you need to cook five tablespoons of rice in a small amount of water until it has the consistency of a slurry porridge. Mix the resulting rice porridge with a glass of skim milk and mashed ripe banana. In case of exacerbation of the disease, you should consume this dish twice a day on an empty stomach.
- Wheat decoction
To prepare the decoction you will need:
- 1 tablespoon of whole wheat grains;
- 200 ml water.
Wheat decoction can also be used for enemas.
- Turnip decoction
To prepare this remedy you will need:
- a few turnip leaves;
- vegetable juice (from the same turnip, or from carrots, zucchini, cabbage, etc.).
This decoction contains ingredients that prevent constipation, improve digestion, and soften stool.
- Decoction of watermelon rinds
What is the prognosis for patients with UC?
The likelihood of curing ulcerative colitis depends on the severity of the disease, the presence of complications, and the timeliness of starting treatment.In the absence of adequate treatment, patients suffering from ulcerative colitis very quickly develop secondary diseases (complications), such as:
- Severe intestinal bleeding;
- Perforation (perforation) of the colon with subsequent development of peritonitis;
- Formation of abscesses (ulcers) and fistulas;
- Severe dehydration;
- Sepsis (“blood poisoning”);
- Liver dystrophy;
- The formation of kidney stones due to impaired absorption of fluid from the intestine;
- Increased risk of developing colon cancer.
However, with mild to moderate, uncomplicated course of the disease, with timely treatment started using all modern methods, with the patient following a diet and preventive measures, the prognosis of the disease is quite favorable. Relapses after proper treatment occur every few years and are quickly stopped with the use of medicines.
How to treat UC with herbs?
Here are some recipes to use medicinal plants in the treatment of nonspecific ulcerative colitis:- Oak bark infusion
To prepare the infusion, a teaspoon of crushed dry oak bark is poured with half a liter of cold boiled water and infused at room temperature for 8-9 hours. Drink the resulting infusion throughout the day in equal portions.
- Aloe vera juice
- Goldenrod infusion
The infusion is prepared as follows: 20 g of dry goldenrod herb, poured with a glass of boiling water, is kept in a boiling water bath for 15 minutes. Then the fire is turned off, but the infusion is not removed from the water bath for another 45 minutes. After this, the infusion is filtered and boiled water is added to 200 ml. Take 2 tablets three times a day. spoons before meals.
- Horsetail infusion
- Chinese bitter gourd infusion
To prepare the infusion you will need:
- 1 tablespoon dry crushed bitter gourd leaves;
- 200 ml of boiling water.
- Herbal infusion
Colitis is a fairly common disease that mainly affects older people. This is an extremely unpleasant disease that significantly impairs a person’s quality of life. If left untreated, the inflammatory process can lead to a lot of unpleasant consequences.
That is why people are quite often interested in the question of what such an illness is. What are the first symptoms of inflammation? When should you see a doctor immediately? What treatment does it offer? modern medicine? Are there any means of prevention? This information will be useful to many readers. So, next we will look at the different types of intestinal colitis and their treatment.
What is colitis?
Colitis is an inflammatory disease that affects the large intestine. According to statistics, men aged 40 to 60 years most often suffer from this disease, and for women the age threshold is even lowered: even twenty-year-olds are among the patients.
Today there are many varieties of this disease. The reasons for it may be different. For the most part, the inflammatory process is associated with the activity of bacterial microorganisms and viruses. Risk factors also include malfunctions, insufficient blood supply to intestinal tissues (observed with high blood pressure, vasospasm, diabetes mellitus, atherosclerosis), as well as poor nutrition(fiber deficiency), bad habits (smoking), the presence of infections in other parts digestive system. In addition, there is also some genetic predisposition.
In most cases, colitis responds quite well to drug treatment, especially if therapy was started in a timely manner. That is why it is important to know about the main causes and first symptoms of the disease.

The main types of intestinal colitis and the causes of their occurrence
Unfortunately, this disease cannot be called rare. It is not surprising that many patients are interested in additional information about the disease. One of the most frequently asked questions: “What is ulcerative colitis of the intestine?” and the reasons for the development of pathology also do not remain aside. However, it's worth knowing that there are dozens of different forms of intestinal inflammation and several commonly used classification systems.
For example, depending on the course of the disease, acute (symptoms are pronounced and appear quickly, intestinal inflammation is often associated with gastritis or enteritis) and chronic colitis (symptoms either fade or worsen).
Depending on the location of the inflammatory process, forms such as proctitis (inflammation of the rectum), sigmoiditis (affected transversitis (transverse colon)) and typhlitis (inflammation of the entire large intestine become inflamed in some cases - this condition is called pancolitis. In addition, simultaneous damage to several departments is possible.
Depending on the causes of the development of the disease, it is customary to distinguish the following types:
- Infectious colitis. Develops against the background of bacterial microflora activity. The disease can be caused by streptococci or staphylococci. An infection can enter the digestive system from the outside, for example, colitis develops against the background of dysentery. In addition, inflammation occurs against the background of a decrease in the activity of the immune system, as a result of which the intensive reproduction of opportunistic microflora begins.
- Ischemic colitis. It develops when the normal blood supply to the large intestine is disrupted, which is observed, for example, with atherosclerosis of the branches of the abdominal aorta.
- People with chronic radiation sickness develop what is called radiation colitis.
- There is also a toxic form of colitis, which is caused by exposure to toxins or medications. For example, quite often uncontrolled use of non-steroidal anti-inflammatory drugs leads to inflammation of the intestinal mucosa and other organs of the digestive tract.
- Quite common and dangerous is ulcerative colitis, which is accompanied by the formation of ulcers on the intestinal walls. Unfortunately, the exact etiology of this disease is unknown - scientists were able to find out that the autoimmune process, genetic inheritance and certain infectious agents play a role in the formation of the disease.
Naturally, there are other classification schemes, as well as forms of inflammation. For example, colitis can develop against the background of allergies. In addition, erosion of the mucous membrane or its gradual atrophy may develop in parallel.
What symptoms are accompanied by acute colitis?
As you can see, there are a variety of types of intestinal colitis. Symptoms of acute forms for the most part look the same, regardless of the form of the disease, so it is worth familiarizing yourself with them.

Often, an acute inflammatory process begins with an increase in temperature and the appearance of signs of general intoxication of the body. In particular, patients complain of weakness, body aches, muscle pain, headache, loss of appetite, and chills.
There are also more specific symptoms that accompany colitis. How does this disease manifest itself? First of all, disorders of the digestive system. In particular, many patients complain of severe sharp pain in the abdomen, especially in the navel area. Often any food intake is accompanied by rumbling and bloating.
A feature of inflammation of the large intestine is constant diarrhea - bowel movements become more frequent up to 5-6 times a day. Often patients feel the urge immediately after eating, in the morning, or even wake up at night. Feces, as a rule, are relatively liquid and foul-smelling, which is associated with the activity of intestinal bacteria.
There are some quite dangerous symptoms of ulcerative colitis of the intestines. In particular, if there is serious damage to the mucous membrane, blood may appear in the stool. If unchanged blood appears constantly, you must tell your doctor about it.
Chronic colitis and features of its course
Chronic intestinal colitis is a rather dangerous disease. Periods of exacerbation are followed by periods of relative calm, when a person feels normal and therefore does not believe that he needs medical help. Moreover, chronic form diseases are much more difficult to treat.
This disease is also accompanied by disturbances in the digestive processes. Patients often suffer from problems with stool - diarrhea is often replaced by constipation, and vice versa. Sometimes the act of defecation is accompanied by abdominal pain. In addition, the inflammatory process can spread to other parts of the digestive system.
It is worth noting that in the absence of treatment, gradual changes are observed in all organ systems. Sick people lose their appetite, resulting in weight loss. In addition, food is not completely absorbed, which gradually leads to the development of anemia, hypo- and avitaminosis, disruption of the normal balance of electrolytes, and exhaustion. The disease also affects emotional state person - there is depression, worsening mood, increased irritability, sleep problems, constant fatigue. Therefore, under no circumstances should you ignore the problem.
Modern diagnostic methods
What should you do if you are worried about symptoms resembling colitis? What to do in such cases? Of course, the first thing you need to do is see a doctor. The fact is that the same symptoms can mask other, more serious diseases, including cancer.
First, the doctor must collect a complete medical history. He will probably ask about the symptoms present, their intensity, time of occurrence, etc. These facts are very important, so be sure to provide the specialist with all the necessary information.
This is followed by a standard inspection. The doctor will palpate the abdomen to look for abnormally enlarged organs. If colitis is suspected, it is necessary for a specialist to quickly detect swelling or swelling in the rectum.
The patient is also required to undergo blood tests (to detect inflammation, hidden bleeding, bleeding disorders) and stool tests (infection or blood impurities can be detected). The results of laboratory tests in this case are very informative.
If necessary, sigmoidoscopy and colonoscopy are prescribed - these studies help to carefully examine the mucous membrane of the large intestine. If the causes of colitis cannot be determined, or there is a suspicion of a malignant process, a biopsy is also performed during the examination - tissue collection with further laboratory testing of samples.
There are some other studies that help not only to detect colitis, but also to assess the degree of damage to the mucosa, find out the location of the inflammatory process, etc. For example, an X-ray examination with a barium enema allows the doctor to study the anatomy and assess the condition of the large intestine. Patients are often advised to computed tomography, which allows a specialist to make a specific diagnosis by assessing the characteristics of the inflammatory process.
In any case, during the diagnostic process it is important not only to find out whether the patient has colitis. The causes, degree of damage, location, stage of development - all these are no less important points on which the choice of treatment regimen directly depends.

Drug treatments
What to do after you are diagnosed with colitis? Only a doctor knows how to treat it, so in no case should you try to cope with the problem yourself. The choice of drugs directly depends on the cause of the disease.
For example, with an infectious form of the disease, it is necessary to take antibacterial agents. Treatment of ulcerative colitis of the intestine involves the use of a whole range of medications. In particular, aminosalicylates and glucocorticoids (hormonal substances that inhibit the inflammatory process) are used.
If an autoimmune reaction is suspected, cytostatics are used - drugs that inhibit the activity of the immune system. Quite often, patients are prescribed to take Mercaptopurine, Methotrexane, Azathioprine and other drugs.
Naturally, symptomatic treatment is also an important part. If there is severe pain, analgesics are prescribed to help alleviate the patient's condition. Antispasmodic drugs, in particular Papaverine and No-Shpa, help restore normal intestinal motility. In the presence of severe diarrhea, Loperamide or other antidiarrheal drugs are prescribed. The presence of bleeding requires taking hemostatic drugs, for example, Tranexam or Dicynon.
In some cases, additional measures are required. For example, with severe digestive disorders, patients are advised to administer intravenous nutrients. Persistent diarrhea can lead to dehydration, so patients are given mineral solutions to help maintain fluid and electrolyte balance.
It is immediately worth noting that the decision on hospitalization is made by the doctor. In mild cases, treatment at home is possible, but only if all recommendations of the treating specialist are followed. If the patient is in serious condition (intestinal bleeding, dehydration, exhaustion), then he must be constantly monitored medical personnel— such restorative therapy can only be carried out in a hospital setting.

When is surgery necessary?
Unfortunately, conservative treatment of ulcerative colitis of the intestine (or any other types of this disease) is not always effective enough. In such cases, surgical intervention is required.
The indication for surgery is the ineffectiveness of drug therapy for severe forms of the disease. In addition, the surgical procedure is performed if the patient develops so-called “emergency” conditions that are life-threatening. In particular, this is toxic dilatation, the onset of malignant tissue degeneration, as well as massive bleeding, etc.
Quite often radical procedures are performed in which the colon. In some cases, doctors place a permanent ileostomy on the anterior abdominal wall to allow for emptying, while preserving the intestinal stump. Unfortunately, such treatment leads to loss of the ability to have anal bowel movements, resulting in patients becoming disabled. Partial removal intestines is also performed, but the percentage of relapses is very high among patients.
How are chronic forms of the disease treated?
Unfortunately, getting rid of chronic inflammation is very difficult. Therefore, therapy in this case is symptomatic, and is aimed at maintaining normal intestinal function and preventing complications.
During periods of exacerbation, which, by the way, are accompanied by almost the same symptoms as acute forms, patients are prescribed anti-inflammatory, antidiarrheal, and painkillers. It is also extremely important to provide the body with the necessary amount of fluid to prevent dehydration.
During periods of remission, proper diet comes to the forefront of therapy. In particular, you need to exclude foods that irritate the intestinal mucosa. In addition, doctors recommend eating only warm food (the same applies to drinks). But during exacerbations, the diet should be more strict. In addition, some doctors prescribe patients periodic intake of vitamin-mineral complexes, which help prevent the development of vitamin deficiencies and also normalize the functioning of the immune system.

Proper diet is an important part of therapy
Today, many people are interested in questions about what ulcerative colitis actually is. We have already discussed the symptoms, treatment and causes of this disease. But it is also worth understanding that proper nutrition is an integral part of therapy. Moreover, in severe forms of the disease and chronic inflammatory processes, a special diet must be followed even after the end of the course of treatment.
Colitis is an inflammation of the intestines, which consequently affects the digestive processes. That is why the diet for such a disease must be gentle. To begin with, it should be noted that all dishes should be either steamed or boiled (the diet can be slightly varied with baked foods). Patients are recommended to eat fractional meals - they need to eat often (sometimes up to 7-8 times a day), but in small portions to prevent stagnation and fermentation of food in the large intestine. By the way, the last meal should be no later than 7 pm.
It is imperative to include a sufficient amount of animal protein in the diet - these can be eggs, lean meats (for example, poultry, veal, rabbit), but in no case fried foods.
There are some categories of foods that irritate the intestinal lining, leading to increased symptoms. Such food should be completely excluded from the diet. In particular, patients are prohibited from eating fatty meats, raw vegetables (fiber, of course, is necessary, but vegetables must be boiled), as well as legumes, corn, mushrooms, and spices. The menu should not include fried, fatty or salty dishes. Prohibited foods also include sunflower seeds, carbonated drinks, alcohol, dried apricots and prunes.
If the patient does not suffer from excess weight, then the diet must be high-calorie (at least 2-3 thousand kcal per day) in order to avoid sudden weight loss.
Intestinal colitis: treatment with folk remedies
Of course, many people are interested in questions about whether there are any other ways to get rid of such a disease. Is it possible to cure, for example, ulcerative colitis at home?
Treatment with folk remedies, of course, exists. But here you need to be very careful. Firstly, before starting to use any home remedy, be sure to consult your doctor - only he can assess the possible benefits or harms.
In most cases, traditional healers recommend taking a decoction of chamomile, sage and centaury. To prepare it, you need to take one teaspoon of dry herbs from each plant, mix and pour a glass of boiling water. After the herbs have infused, the liquid can be strained. It is recommended to take one tablespoon every two hours. The duration of the course of treatment should be at least a month - only then the visible results of such therapy will begin to appear.
There are other recipes. For example, dried watermelon rinds are considered beneficial for colitis. 100 g of crusts need to be poured with 400 ml of boiling water and allowed to brew. You need to drink half a glass 4 to 6 times a day. In addition, you can prepare a decoction of pomegranate peels. 2 g of dry crusts should be poured with a glass of water and boiled over low heat for half an hour. It is recommended to take two tablespoons twice a day.
In any case, it is tedious to understand that traditional treatment of colitis is possible only as an auxiliary method and in no case can replace full-fledged drug therapy.
Prevention of colitis
Colitis is a very common inflammatory disease, and, unfortunately, no specific preventive measures exist today. Naturally, you can follow certain rules that will help reduce the risk of developing the disease. In particular, you need to carefully monitor the quality of the food and water you consume, follow all food preparation rules, adhere to basic sanitary and hygienic standards, wash your hands before eating, etc.
Since the development of colitis is often associated with an abnormal immune response of the body, you need to take care of the state of the immune system. An integral part of any prevention is a proper diet rich in vitamins and minerals, as well as feasible physical activity.
It has been proven that some types of colitis develop much more often against the background of insufficient blood circulation, so it is extremely important to observe the prevention of diseases such as atherosclerosis and hypertension, and also to stop smoking.
If you have the first alarming signs, you should immediately consult a doctor: the sooner the disease is diagnosed and adequate therapy is started, the easier it will be to get rid of the disease without any serious complications.
Nonspecific ulcerative colitis (UC) is a chronic disease of the gastrointestinal tract of a recurrent nature, in which the mucous membrane of the large intestine becomes inflamed, on which ulcers and areas of necrosis form.
Clinically, ulcerative colitis is manifested by bloody diarrhea, arthritis, weight loss, general weakness, abdominal pain, and this disease increases the risk of developing colorectal cancer. We will tell you more about ulcerative colitis of the intestine - symptoms and treatment of the disease in this article.
Causes of Ulcerative Colitis
The etiology of the disease is considered not fully understood; scientists are still intensively searching for the true causes of ulcerative colitis. However, the main risk factors for this disease are known, which include:
American experts conducted a large-scale study and found that fungi in the human intestine are associated with inflammatory bowel diseases (Crohn's disease and ulcerative colitis), reports the Los Angeles Times. Experiments conducted on rodents allowed scientists to prove the connection between more than 100 species of various fungi found in their intestines and ulcerative colitis of the intestine.
The presence of fungi in the body of mammals activates the production of dectin-1 protein by leukocytes. In the case where the body in mice could not produce it, the mice become more susceptible to the development of ulcerative colitis than their healthy counterparts. Moreover, the use of antifungal drugs can mitigate the course of this disease in rodents.
In humans, Dectin-1 is encoded by the CLEC7A gene; based on these studies, it turned out that in the presence of a mutant form of this gene, the patient developed ulcerative colitis, which was not amenable to traditional methods of treatment (diet, NSAIDs, corticosteroids). Mutations in the CLEC7A gene contribute to the development of a more severe form of colitis, since this gene is associated with other factors that influence inflammation, and antifungal treatment in this case helps to improve the patient's condition.
Symptoms of Ulcerative Colitis
There are main symptoms of ulcerative colitis associated with the gastrointestinal tract (intestinal manifestations) and extraintestinal symptoms.
The main intestinal symptoms of UC are:
- Bloody diarrhea
Diarrhea with blood and mucus (and sometimes even pus) is the main diagnostic sign of the disease. Sometimes the discharge of blood, mucus and pus occurs spontaneously (not during bowel movements). The frequency of bowel movements in patients with UC varies - from several times a day to 15 - 20 times (severe cases). The frequency of stool increases in the morning and at night.
- Pain in the projection of the abdomen
The pain may also have varying degrees intensity - from weak to sharply expressed, accompanied by extreme discomfort. Most often, the pain is localized in the left half of the abdomen. Severe abdominal pain that is not relieved by taking analgesics is a sign of complications of the disease.
- Increase in temperature to low-grade levels.
- Other signs of intoxication of the body: weakness, weight loss, poor appetite, frequent dizziness.
- False urge to defecate (tenesmus). Sometimes a patient may discharge only a fragment of mucus or mucus with pus instead of feces (symptom of “rectal spitting”).
- Bloating ().
- Possible fecal incontinence.
- Sometimes, instead of diarrhea, the patient develops constipation, which is a sign of severe inflammation of the colon mucosa.
- The likelihood of rapid (fulminant, fulminant) development of ulcerative colitis.
This form develops in just a few days, its manifestation is toxic megacolon (expansion or dilatation of the lumen of the large intestine). At the same time, the patient’s temperature rises sharply, reaching over 38°C. The patient is weak, adynamic, rapidly losing weight, he experiences abdominal pain, frequent loose stools with copious amounts of mucus, blood and pus, and abdominal pain. In the terminal stage of UC, tachycardia occurs and decreases arterial pressure, oliguria appears. The patient has bloating and tenderness of the abdomen, bowel sounds are not heard. Neutrophilic leukocytosis is noted in the blood, and a dilated colon is visible on the x-ray (its diameter exceeds 6 cm). Dilatation of the large intestine is caused by an increase in nitric oxide, which increases the contractile function of intestinal smooth muscles. Excessive expansion of the large intestine is dangerous due to perforation of its wall (rupture).
Extraintestinal manifestations of UC
They occur infrequently - in only 10 - 20% of patients. These include:
- Skin lesions in the form of erythema nodosum and pyoderma gangrenosum, which is associated with the presence in the blood of an increased concentration of bacterial antigens, immune complexes, and cryoproteins.
- Symptoms of damage to the oropharynx. Occurs in 10% of patients. They are associated with the appearance of aphthae - specific rashes on the mucous membrane oral cavity, the number of which decreases as the disease goes into remission.
- Eye damage (occurs even less frequently - in only 5 - 8% of cases), they manifest themselves as: uveitis, episcleritis, conjunctivitis, retrobulbar neuritis, keratitis, choroiditis.
- Articular lesions. Inflammatory processes in the joints are of the nature of arthritis (most common), sacroiliitis, spondylitis. These lesions can be combined with intestinal pathology or precede the main symptoms of ulcerative colitis.
- Pathology of the skeletal system in the form of: osteoporosis (increased bone fragility), osteomalacia (softening of bones), aseptic and ischemic necrosis.
- Damage to the pulmonary system (occurs in 35% of patients with UC).
- Damage to the pancreas, liver and bile ducts. These changes are caused by disturbances in the functioning of the endocrine system.
- The rarest extraintestinal symptoms of ulcerative colitis of the intestine are: and glomerulonephritis.
Ulcerative colitis has an acute phase and a remission phase. The disease begins gradually at first, but quickly gains momentum when the signs of ulcerative colitis become more pronounced.
Sometimes the symptoms weaken, but then intensify again. With constant treatment, the disease takes on the character of recurrent chronic ulcerative colitis, the symptoms of which weaken with long-term remission. The frequency of relapses in patients with nonspecific ulcerative colitis most often depends not on the degree of intestinal damage, but on supportive treatment (non-steroidal anti-inflammatory drugs, antibacterial, antiviral agents).
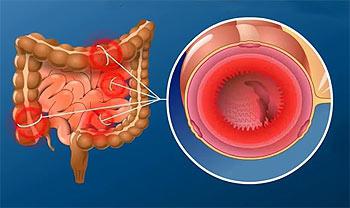
During the acute phase of the disease, the large intestine looks like this: hyperemia and swelling of its mucosa occur, intestinal bleeding and ulcers appear. The process of remission, on the contrary, is accompanied by atrophic changes in the mucous membrane - it becomes thinner, its function is impaired, and lymphatic infiltrates appear.
Diagnosis of the disease
The diagnosis and treatment of ulcerative colitis is carried out by a therapeutic specialist or gastroenterologist. Suspicion of the disease is caused by a complex of corresponding symptoms:
- diarrhea mixed with blood, mucus and pus
- abdominal pain; arthritis
- eye disorders due to general intoxication of the body
Laboratory diagnostics.
- In a general blood test, a patient with ulcerative colitis shows anemia (a decrease in the number of red blood cells and hemoglobin), and there is leukocytosis. In a blood test for biochemistry, an increase in the blood content of C-reactive protein is noted, which is an indicator of the presence of inflammation in the human body. In addition, the concentration of albumin, magnesium, calcium decreases, and the amount of gamaglobulins increases, which is associated with the active production of antibodies.
- In an immunological blood test, most patients show an increase in the concentration of cytoplasmic antineutrophil antibodies (they appear due to an abnormal immune response).
- A stool analysis of a patient with ulcerative colitis shows blood, pus and mucus. Pathogenic microflora is sown in feces.
Instrumental diagnosis of UC.
Endoscopy (rectosigmoidoscopy, reveals in the patient a complex of symptoms characteristic of the disease:
- swelling and hyperemia, granulosa of the mucous membrane
- pseudopolyps
- contact bleeding
- the presence of pus, blood and mucus in the intestinal lumen
- During the remission phase, pronounced atrophy of the mucous membrane of the large intestine is observed.
("video pill") in the near future, it will be performed on those patients who, due to the pain of the procedure and discomfort, refuse to undergo a colonoscopy. However, capsule endoscopy will not replace traditional endoscopic examination, since the image quality is inferior to direct visualization. The approximate cost of such a capsule will be about $500.
X-ray examination is also an effective method for diagnosing ulcerative colitis. In this case, a barium mixture is used as a contrast. On x-ray In a patient with UC, there is a noticeable expansion of the intestinal lumen, the presence of polyps, ulcers, and shortening of the intestine. This type examination helps prevent intestinal perforation.
Treatment of ulcerative colitis
There is no etiological treatment that can address the cause of ulcerative colitis. Treatment of the disease is symptomatic and is aimed at: eliminating the inflammation process, maintaining remission and preventing complications. If drug therapy does not have an effect, the patient is indicated for surgical treatment.
Conservative treatment methods for UC include:
Diet therapy. During periods of exacerbation, the patient is advised to refrain from eating. You can only drink water. During the period of remission, the patient is recommended to reduce the amount of fat in the diet and increase the protein content ( lean fish and meat, cottage cheese, eggs). It is recommended to avoid coarse fibrous fiber, which can injure the delicate intestinal mucosa. The following carbohydrates are recommended: porridge, honey, jelly, jelly, berry and fruit compotes and decoctions. The patient is recommended to take vitamins: A, K, C, as well as calcium. IN severe cases artificial nutrition is recommended - parenteral and enteral.
NSAIDs (non-steroidal anti-inflammatory drugs) salofalk, mesalazine, sulfasalazine and corticosteroids - prednisolone, methylprednisolone. The dosage of drugs is selected by the doctor individually.
Antibiotics. In case of exacerbation of the disease, antibiotics are also recommended: ciprofloxacin, tsifran, ceftriaxone, tienam.
Surgical intervention
Surgical treatment of ulcerative colitis is indicated for patients who do not respond to conservative methods. Indications for surgery for ulcerative colitis are:
- perforation (perforation of the intestinal wall);
- signs of intestinal obstruction;
- abscess;
- presence of toxic megacolon;
- profuse bleeding;
- fistulas;
- bowel cancer.
Main types surgical intervention are:
- Colectomy (excision of the colon).
- Proctocolectomy (removal of the rectum and colon) with preservation of the anus.
- Proctocolectomy followed by ileostomy. In this case, the rectum and colon are excised, after which an ileostomy (permanent or temporary) is applied, through which natural waste is removed from the human body. Subsequently, the patient undergoes reconstructive surgery, the ileostomy is removed and the natural path of defecation is restored.
Ulcerative colitis is a chronic inflammatory process in the mucous membrane of the colon, accompanied by the appearance of non-healing ulcers, areas of necrosis and bleeding. This pathology differs from simple inflammation. With it, ulcerative defects form on the colon mucosa. Prolonged course of the disease increases the likelihood of developing cancer.
Therefore, at the slightest suspicion of this disease, you should consult a doctor who will recommend correct treatment ulcerative colitis with the help of medications and folk remedies.
What is ulcerative colitis?
Ulcerative colitis is a chronic inflammatory disease of the colon mucosa resulting from an interaction between genetic and environmental factors, characterized by exacerbations. UC affects the rectum, gradually spreading continuously or immediately affecting the rest of the colon. This disease is also called nonspecific ulcerative colitis (UC).
Usually occurs in adults aged 20 to 35 years or after 60. In children, this disease occurs extremely rarely and accounts for only 10-15% of cases of all identified pathologies. At the same time, girls are at greatest risk of developing the disease among adolescents, and in the preschool and primary school period, on the contrary, boys are.
Ulcerative colitis is classified:
- By clinical course- typical and fulmicant; chronic form (recurrent and continuous);
- localization - distal (proctitis, proctosigmoiditis); left-sided (to the middle of the transverse colon); subtotal; total (pancolitis); total with reflux ileitis (against the background of total ileitis, a section of the ileum is involved in the process);
- severity of clinical manifestations.
Pathological anatomy (morphological substrate of the disease) of ulcerative nonspecific colitis represented by diffuse superficial damage to the walls of the large intestine. In the vast majority of cases the disease is localized in the terminal (final) parts of the large intestine: sigmoid and rectum. Involvement of the entire large intestine is much less common. Involvement of the final portion of the small intestine is very rare.
Causes
Unfortunately, the exact etiology of this disease is unknown - scientists were able to find out that the autoimmune process, genetic inheritance and certain infectious agents play a role in the formation of the disease.
Residents of cities in developed countries are more susceptible to ulcerative colitis. As a rule, the disease develops either in young people or in those over 60, although in fact a person of any age can get this disease.
It has been suggested that it may be provoked by:
- some unspecified infection (but ulcerative colitis is not contagious);
- unbalanced diet (fast food, diet lacking fiber, etc.);
- genetic mutations;
- medications (non-hormonal anti-inflammatory drugs, contraceptives, etc.);
- stress;
- changes in intestinal microflora.
Under the influence of these factors, symptoms of ulcerative colitis develop as a result of autoimmune processes in the body.
Symptoms of ulcerative colitis of the intestine
Ulcerative colitis has an acute phase and a remission phase. The disease begins gradually at first, but quickly gains momentum when the symptoms become more pronounced.

Symptoms of ulcerative colitis from the digestive system:
- cramping pain in the abdomen localized predominantly on the left, which is difficult to relieve with medications;
- diarrhea or loose stools mixed with mucus, blood or pus, worse at night or in the morning;
- constipation that replaces diarrhea, which is caused by intestinal spasm;
- bloating();
- frequent false urge to defecate (tenesmus), which occurs due to retention of feces above the area with inflammation;
- spontaneous release of mucus, pus and blood (not during defecation) as a result of imperative (irresistible) urges.
In 10% of cases, in addition to the mentioned intestinal and common symptoms extraintestinal manifestations occur:
- joint lesions;
- various rashes on the skin and mucous membranes (for example, in the mouth);
- eye disorders;
- damage to the liver and bile ducts;
- thrombus formation, etc.
They may precede intestinal disorders. The severity of extraintestinal manifestations sometimes depends on the activity of the inflammatory lesion of the intestine, and in some cases is completely unrelated to it.
With mild ulcerative colitis, patients complain of cramping pain or discomfort in the abdomen, weakness. Semi-liquid stools are possible 2-4 times a day with a small admixture of blood and mucus.
If ulcerative colitis is more severe, then loose stools occur up to 8 times a day with a significant admixture of mucus, blood and pus. With this form of the disease the following are noted:
- pain in the abdomen, often in the area of the left half (flank).
- there is weakness,
- slight fever
- weight loss.
- may be tachycardia,
- pain in the liver.

Symptoms during an exacerbation
During the period of exacerbation, symptoms of intoxication appear:
- fever,
- weakness,
- malaise.
A distinctive sign of ulcerative colitis from simple catarrhal disease is weight loss. Patients often look exhausted. Their appetite is reduced. With intestinal colitis, ulcerative defects are formed. They may bleed as stool passes.
Symptoms may become weaker and then worsen again. If continuous treatment is carried out, a remission phase begins and the symptoms subside. How often relapses occur is determined by the treatment, and not by how damaged the intestines are.
Consequences and possible complications
In the absence of drug therapy and non-compliance with the diet, complications may develop. In this case, the symptoms of ulcerative colitis become more pronounced. Possible the following consequences inflammation of the large intestine:
- massive bleeding;
- toxic dilatation of the intestine (formation of megacolon);
- perforation;
- malignancy of ulcers;
- joint inflammation;
- damage to internal organs (gallbladder, liver, skin).
Diagnostics
The diagnosis and treatment of ulcerative colitis is carried out by a therapeutic specialist or gastroenterologist. Suspicion of the disease is caused by a complex of corresponding symptoms:
- diarrhea mixed with blood, mucus and pus
- abdominal pain;
- arthritis, eye disorders due to general intoxication of the body.
Laboratory diagnostic methods:
- clinical blood test (increased quantity and ESR, decreased level of hemoglobin and red blood cells);
- biochemical blood test (increased levels C-reactive protein and immunoglobulins);
- biopsy - histological examination of tissue samples;
- stool analysis for fecal calprotectin is a special marker for diagnosing intestinal diseases, which in ulcerative colitis can increase to 100 - 150;
- coprogram (presence of occult blood, leukocytes and erythrocytes).
If the results of the tests confirm presence of the disease, the doctor prescribes an instrumental examination. An endoscopy is performed to detect possible swelling in the mucous membrane, the presence of pseudopolyps, pus, mucus, blood in the intestines and determine the extent of organ damage.
Endoscopic examinations (colonoscopy, rectosigmoidoscopy) make it possible to identify a complex of symptoms characteristic of the pathology in the patient:
- the presence of mucus, blood, pus in the intestinal lumen;
- contact bleeding;
- pseudopolyps;
- granulosa, hyperemia and swelling of the mucous membrane;
- in the remission phase, atrophy of the intestinal mucosa is noted.
X-ray examination also applies to effective methods for the diagnosis of ulcerative colitis. A barium mixture is used as a contrast agent in this procedure. An X-ray of a patient with ulcerative colitis clearly visualizes expansion in the lumen of the large intestine, shortening of the intestine, and the presence of ulcers and polyps.
Treatment of ulcerative colitis
Treatment will be symptomatic, it should eliminate the inflammation process and maintain remission, as well as prevent complications. If medications are not effective, surgery may be indicated.

The objectives of treating a patient with UC are:
- achieving and maintaining remission (clinical, endoscopic, histological),
- minimizing indications for surgical treatment,
- reduction in the incidence of complications and side effects drug therapy,
- reduction in hospitalization time and treatment costs,
- improving the patient's quality of life.
The results of treatment largely depend not only on the efforts and qualifications of the doctor, but also on the willpower of the patient, who clearly follows medical recommendations. The modern equipment available in the doctor’s arsenal medications allow many patients to return to normal life.
Medications
To make these goals a reality, experts prescribe the following treatment methods for patients with intestinal ulcerative colitis:
- taking non-steroidal anti-inflammatory drugs, for example, Salofalk, Dipentum, Sulfasalazine;
- use of corticosteroids (Metyprednisolone, Prednisolone);
- antibacterial therapy through the use of drugs such as Tienama, Cifran, Ciprofloxacin, Ceftriaxone;
- taking immunomodulators (Azathioprine, Cyclosporine, Infliximab, Methotrexate);
- consumption of calcium and vitamins A, C, K.
In case of development purulent complications or the addition of an infection, systemic antibacterial drugs. Medicines alone cannot cure a person. In the remission phase, in the absence of pain and bleeding, physiotherapeutic procedures are prescribed. Most often carried out:
- Exposure to alternating current.
- Diadynamic therapy.
- Interference therapy.
Patients with mild and moderate variants of ulcerative colitis can be treated on an outpatient basis. Severe patients must be examined and treated in a hospital, since both diagnostic and therapeutic interventions can have serious and even life-threatening complications.
With proper implementation of the doctor’s recommendations, daily adherence to dietary instructions, as well as supportive therapy, it is possible to significantly increase the time of remission and improve the patient’s quality of life, but, unfortunately, complete recovery cannot be achieved when treating this disease.
Operation
Surgical treatment of ulcerative colitis is indicated for patients who do not respond to conservative methods. Indications for surgery are:
- perforation (perforation of the intestinal wall);
- signs of intestinal obstruction;
- abscess;
- presence of toxic megacolon;
- profuse bleeding;
- fistulas;
- bowel cancer.
It is possible to treat ulcerative intestinal colitis surgically today in the following ways:
- through partial or total colectomy - excision of the colon;
- using proctocolectomy - removal of the colon and rectum leaving the anus;
- through a proctocolectomy and a temporary or permanent ileostomy, through which natural waste is removed from the body.
It is necessary to pay attention to possible physical and emotional problems after surgical treatment; care should be taken to ensure that the patient receives everything necessary instructions before and after surgical intervention and provide him with all possible medical and psychological support.
Knowing exactly what ulcerative colitis is and how to treat it, we can say with confidence that the prognosis of the disease is quite favorable. The pathological process is curable thanks to modern methods therapy. Most patients experience complete remission, and only 10% of cases retain mild clinical symptoms.
Diet and proper nutrition

With this disease, normalization of nutrition is of paramount importance. The diet for ulcerative colitis is aimed at mechanical, thermal and chemical sparing of the colon mucosa.
- The diet is based on the consumption of chopped, soft food, steamed or boiled.
- You should forever forget about hot sauces, fatty seasonings, alcohol, and cigarettes.
- Fruits and vegetables should be consumed only in heat-treated form, because in their raw form they contain a lot of fiber, which negatively affects the functioning of the affected intestines.
- During an exacerbation, the diet includes liquid and pureed porridge (rice, semolina) in water (milk and broths are excluded). Buckwheat enhances motor skills, so it is not recommended during exacerbation. It is convenient to use porridge for baby food, but it needs to be diluted by half with water.
| Authorized products: | For ulcerative colitis, you need from the diet exclude the following foods and dishes: |
|
|
To find out exactly what foods you are allowed to eat, consult your doctor.
Menu for ulcerative colitis for the day
A diet for ulcerative colitis of the intestine can be implemented through the following menu option.
- Breakfast: cereal porridge with 1 tsp. melted butter, steam cutlet, rosehip decoction.
- Lunch: curd mass, berry jelly.
- Lunch: potato soup with meatballs, rice and minced meat casserole, compote.
- Afternoon snack: green tea, crackers.
- Dinner: stewed vegetables, fish cutlet, tea.
- Before bed: kefir/baked apple.
This menu option is suitable for the period after an exacerbation. Additionally, you can eat 200-250 grams of dried bread, 1 glass of jelly or compote.
A diet for ulcerative colitis of the colon, including the rectum, leads to a number of positive changes:
- promotes speedy recovery normal stool, eliminating diarrhea or constipation;
- increases the effectiveness of medications, as it compensates for protein losses, accelerates the healing of the mucous membrane, due to which a number of medications begin to act more actively;
- compensates for the loss of nutrients, restores metabolism and energy reserves.
Folk remedies
In therapeutic therapy, it is also allowed to use folk remedies, but only if the disease is at the initial stage of development and the treatment is agreed upon with the doctor. The most effective ways to treat the disease, according to patients, are fasting, refusing to eat animal foods, and switching to a raw food diet. From herbal remedies Decoctions of yarrow, alder cones, wormwood, sage, and potato juice help well.
- 100 g dried watermelon rind pour 2 cups of boiling water, leave and strain. Take 100 g up to 6 times a day. This allows you to relieve inflammation in the intestines in acute and chronic forms of the disease.
- Perfectly relieves inflammatory processes in the intestines potato juice. It is enough to grate a potato, squeeze the juice out of it and drink it half an hour before meals.
- Take an equal amount of peppermint leaf, inflorescences of chamomile, rhizomes of cinquefoil erecta. Infuse 1 tablespoon of the mixture for 30 minutes in 1 glass of boiling water, strain. Take 1 glass 2-3 times a day for colitis.
- Treat symptoms of exacerbation bird cherry helps well. Traditional healers recommend preparing a decoction (one spoonful of flowers per glass of water). Take three times, ¼ cup every day.
Prevention
Prevention of the development of this intestinal pathology consists of proper nutrition and periodic examination. It is important to treat promptly chronic diseases digestive tract. The prognosis for ulcerative colitis in the absence of complications is favorable.
Ulcerative colitis is a serious disease that requires immediate and competent treatment. Do not delay visiting your doctor when the first symptoms appear. It is important to remember that in the event of an acute form of the disease, the organ is affected quickly, which can lead to the development of cancer or various complications.
The long-term prognosis is characterized by an increased risk of colon cancer. The diagnosis is based on colonoscopy findings. Treatment involves the appointment of 5-aminosalicylic acid, corticosteroids, immunomodulators, anticytokine drugs, antibiotics, and in some cases, surgery.
Causes of Ulcerative Colitis
Unknown. It is believed that the cause may be various bacteria, viruses or their metabolic products.
Pathomorphology. The surface of the ulcers is covered with fibrin or purulent contents. The intestinal wall thickens, the intestine narrows, and shortens. When ulcers heal, pseudopolyps are formed, which can lead to the development of colon carcinoma.
Pathophysiology
UC usually begins with damage to the rectum. The process may remain localized at this level (ulcerative proctitis) or spread proximally, sometimes affecting the entire colon. In rare cases, colitis involves a large part of the colon from the very beginning.
Inflammation within UC affects the mucous membrane and submucosal layer, characterized by the presence of a clear boundary between healthy and affected tissue. The muscle layer is affected only in severe cases. IN early stages the mucous membrane is erythematous, the surface is covered with small granules, is easily vulnerable, the normal vascular pattern disappears, scattered hemorrhagic elements are often detected. Severe forms are characterized by large ulcerations of the mucous membrane with copious purulent discharge. Islands of relatively intact or inflamed hyperplastic mucosa (pseudopolyps) protrude above the ulcerated surface. The formation of fistulas and abscesses is not observed.
Toxic, or fulminant, colitis is observed with transmural spread of the ulcerative process. Over the course of several hours or days, the colon loses its ability to maintain tone and begins to expand.
The term "toxic megacolon" can be misleading because... inflammation with intoxication and complications can occur without the development of obvious megacolon (a sign of the latter is an increase in the diameter of the transverse colon > 6 cm during an exacerbation). Toxic colitis - emergency, which usually develops spontaneously with very severe colitis, but can be triggered by taking opioids or antidiarrheal drugs with anticholinergic action. This condition carries the risk of colon perforation, which significantly increases the likelihood of death.
Classification of ulcerative colitis
Ulcerative colitis is classified:
- according to the clinical course - typical and fulmicant; chronic form (recurrent and continuous);
- localization - distal (proctitis, proctosigmoiditis); left-sided (to the middle of the transverse colon); subtotal; total (pancolitis); total with reflux ileitis (against the background of total colitis, the ileum area is involved in the process);
- severity of clinical manifestations.
Symptoms and signs of ulcerative colitis
Bloody diarrhea of varying severity and duration is followed by periods of absence of symptoms. As a rule, the attack begins unexpectedly, with the appearance of an urgent urge to defecate, mild cramping pain in the lower abdomen, and blood and mucus in the stool. In some cases, symptoms of exacerbation develop due to infection (amoebiasis, shigellosis).
At ulcerative lesion In the rectosigmoid region, the stool is normal or dense and dry, but during bowel movements or between episodes of bowel movement there is mucus discharge with blood and leukocytes. There are no systemic manifestations, or they are mild.
With a more proximal spread of the ulcerative process, the stool becomes unformed (frequency > 10 per day, often with severe cramping pain and painful tenesmus that continues at night. The stool may be watery, contain mucus, or consist entirely of blood and pus.
Toxic, or fulminant, colitis manifests with sudden appearance severe diarrhea, fever up to 40 ° C (104 ° F), abdominal pain, signs of peritonitis (in particular, the phenomenon of “rebound pain”), severe intoxication.
Systemic manifestations that are most characteristic of widespread colitis include general weakness, fever, anemia, anorexia, weight loss. Extraintestinal symptoms (especially joint and skin damage) are very characteristic of forms of the disease with pronounced systemic manifestations.
Proctitis is more common than total colitis. When the rectum is involved in the process, the patient complains of constipation and tenesmus.
Extraintestinal manifestations of UC associated with the activity of colitis are peripheral arthropathy, erythema nodosum, episcleritis, aphthous stomatitis, pyoderma gangrenosum, anterior uveitis; not associated with colitis - sacroiliitis, ankylosing spondylitis, primary sclerosing cholangitis; rare manifestations - pericarditis, amyloidosis.
Diagnosis of ulcerative colitis
- Microbiological examination and microscopy of stool (to exclude infectious pathology).
- Sigmoidoscopy with biopsy.
Endoscopic examination reveals swelling, inflammatory infiltration, muco-bloody effusion and contact bleeding. In severe cases, erosions and ulcers are found, the bottom of which is covered with pus.
Beginning of the disease. The presence of a disease can be suspected typical symptoms, especially in combination with extraintestinal manifestations and when indicating previous similar attacks. Ulcerative colitis must be differentiated from Crohn's disease, but more importantly - from other forms of acute colitis (in particular, infectious, ischemic in the elderly).
In each case, a stool culture test for pathogenic intestinal microflora is indicated, and it is also necessary to exclude the presence of Entamoeba histolytica in fresh stool samples. If medical history (epidemiological situation, travel) gives reason to suspect amebiasis, it is necessary to conduct histological and serological studies. Indications of previous antibiotic use or hospital stay necessitate evaluation of stool for the presence of Clostridium difficile toxins. Patients at risk should be tested for HIV infection, gonorrhea, herpes virus infection, chlamydia and amoebiasis. Women may develop colitis induced by oral contraceptives; As a rule, it resolves on its own after stopping the medication.
It is necessary to perform sigmoidoscopy, because This study allows you to confirm the presence of colitis, and take mucus and feces for cultural and microscopic examination, as well as material for histological examination from the affected areas. Although endoscopy and biopsy may not provide diagnostic information ( Various types colitis have similar features), yet acute self-limiting infectious colitis can usually be distinguished from ulcerative colitis and Crohn's disease. Severe perianal lesions, the absence of inflammation in the rectum, bleeding, and the asymmetrical or segmental nature of the lesions of the colon are more in favor of the presence of Crohn's disease than ulcerative colitis. The need for colonoscopy arises in isolated cases when inflammation extends proximal to the level of reaching the sigmoidoscope.
Laboratory tests are carried out to exclude anemia, hypoalbuminemia, and electrolyte metabolism disorders. Liver tests should be assessed; increased activity alkaline phosphatase and angleamyl transpeptidase may indicate the presence of primary sclerosing cholangitis. The presence of antibodies to Saccharomyces cerevisiae is relatively specific for Crohn's disease. However, these studies do not reliably distinguish between UC and CD and are not recommended for use in daily practice. It is also possible to have leukocytosis, thrombocytosis and increased acute phase parameters (ESR, C-reactive protein).
X-ray examination can reveal pathological changes, but it is difficult to make an accurate diagnosis. An X-ray of the abdominal cavity reveals swelling of the mucous membrane, smoothness of the haustra and the absence of formed feces in the affected colon. With irrigoscopy, changes are revealed more clearly, ulcerations can also be detected, but the study cannot be carried out in the acute phase of the disease. After several years of illness, a shortened, rigid colon with mucosal atrophy or the presence of pseudopolyps may be detected. Radiological signs of a “thumbprint” and the segmental nature of the lesion are more characteristic of ischemic colitis or Crohn’s disease.
Fulminant course. In case of severe exacerbation, a more in-depth examination is necessary. X-rays are taken; The images may reveal signs of megacolon - accumulation of gas in the lumen of an extended segment of the intestine, which is in a paralytic state as a result of the loss of the ability of smooth muscle cells to maintain tone. Colonoscopy and irrigoscopy should be avoided due to the risk of perforation. Need to get the result general analysis blood with an assessment of ESR, tests for electrolytes, prothrombin time, partial thromboplastin time, blood group and Rh factor.
The patient's condition should be closely monitored for signs of developing peritonitis or perforation. Grade liver dullness the percussion method makes it possible to identify the first clinical sign of free perforation - the disappearance of dullness, especially in patients receiving high doses of corticosteroids, but “erases” the symptoms of peritoneal irritation. Every 1-2 days, an x-ray of the abdominal cavity is performed to monitor the condition of the dilated area of the intestine and identify free or intramural gas.
Course and prognosis of ulcerative colitis
Ulcerative colitis is a chronic, lifelong inflammatory disease in which the immune system (which normally fights infections) attacks your colon, causing ulcers and bleeding from the lining of the colon. Symptoms usually occur during periods of exacerbation (we call them “attacks” of the disease) and can persist for months and sometimes years. These exacerbations may occur differently in different patients and may be accompanied by abdominal pain, diarrhea, including blood, nausea, vomiting and/or weight loss. This leads to a decrease in quality of life, frequent visits to the doctor and hospitalizations, and in some patients it becomes an indication for removal of the colon due to worsening of the disease. Most patients experience about two exacerbations of the disease within 5 years, but in some patients the disease may progress differently. In many untreated patients, UC tends to progress over time. Exacerbations occur more frequently and become more severe, increasing the likelihood of hospitalization and even surgery to remove the colon (colectomy). In addition, if left untreated, UC patients have an increased risk of developing colon cancer over time.
After establishing a diagnosis, so that exacerbations occur less frequently and are easier, it is recommended to immediately prescribe treatment. Due to the development of new drugs, the likelihood of worsening the disease is now less than it was a couple of decades ago. These treatments also reduced the need to remove the colon (colectomy) and may have reduced the risk of colon cancer. It is important to understand that UC is lifelong and medications cannot cure it, but are extremely effective in controlling the disease.
Ulcerative colitis is a chronic inflammatory disease characterized by repeated acute exacerbations, followed by periods of remission. Previous population-based studies have shown that without treatment, these patients have an increased risk of colorectal cancer (CRC) and mortality, although this risk has decreased in recent decades due to the successful use of immunosuppressants and biological therapies. An uncontrolled disease process can spread throughout the colon, leading to systemic manifestations that may require colectomy.
The course of the disease depending on the extent of the lesion
Depending on the extent of the lesion, ulcerative colitis is divided into ulcerative proctitis, left-sided colitis and widespread (total) colitis. The Montreal classification includes extent of involvement, severity of symptoms (number of bowel movements per day), and signs of systemic disease (erythrocyte sedimentation rate, temperature, hemoglobin). Determining the severity of the disease and the extent of the lesion is convenient for prognosis. Ulcerative proctitis is the most common form of the disease (30-60%), and left-sided (10-40%) and widespread colitis (10-35%) are less common. The risk of proximal disease spread is estimated to be 10-20% over 5 years, rising to 30% over 10 years.
The extent of the lesion is a major determinant of disease spread throughout the intestine, which may reflect disease activity and worsen disease outcome. In patients with ulcerative proctitis, the disease transforms into widespread colitis with a frequency of 14% within 10 years from the date of diagnosis. According to the Norwegian IBSEN study, with left-sided colitis, the incidence of spread of the affected area was higher - 28%. Independent factors predicting proximal disease extension include young age at diagnosis and primary sclerosing cholangitis (PSC) in a prospective study of 420 patients. The average time to transformation of proctitis into left-sided or widespread colitis in this study was 5.25 years.
Expected frequency of exacerbations of the disease
Most patients with UC experience at least 2 exacerbations within 5 years, but less than 1 exacerbation per year on average. In approximately half of the patients included in the Norwegian IBSEN study, the exacerbation at which the diagnosis was made was also the most severe, and in 1/3 subsequent relapses were of the same frequency as the first. Patients with a younger age at diagnosis generally experienced exacerbations more often. Patients who were diagnosed after age 50 were found to have fewer exacerbations and were less likely to undergo colectomy. These patterns were also confirmed in the multicenter IBD study of the European Commission.
Long-term complications
The progression of UC can lead to the formation of benign strictures of the colon due to hypertrophy and irreversible contraction of the muscular layer of the mucosa, which actually separates from the submucosal layer. These strictures cause serious difficulties, since in their presence it is impossible to completely exclude hidden malignant process in the narrowing zone, and therefore they become an indication for surgery. In addition, with a long course of UC, the number of neuroglial cells decreases, which leads to impaired motility and constant diarrhea, despite the healing of the mucous membrane detected by endoscopy, as well as impaired sensitivity of the rectum, accompanied by urgency and incontinence associated with inhibition of the reservoir function of the rectum intestines. These changes may persist even after the mucosa has healed, which may explain why some patients continue to experience symptoms even in the absence of active inflammation.
Risk of Colectomy
Colectomy is an intervention that cures UC and significantly improves overall health, but for some patients, living with an ostomy or J-pouch can be extremely difficult. About 50% of colectomies for UC are performed for urgent indications. Colectomy has not been shown to reduce mortality, but inappropriate refusal of timely surgery increases the incidence postoperative complications and mortality. Colectomy rate in last years decreased: two independent studies showed that the annual rate of colectomy for UC decreased from 9% in 1962-1987. up to 6% in 2003-2005 This decrease appears to be due to more widespread use azathioprine/mercaptopurine recently. In a recently published European Commission IBD study, the mean colectomy rate for UC was 8.7% at 10-year follow-up. Differences in colectomy rates between northern (10.4%) and southern centers (3.9%) suggest that the disease is more severe in patients living in colder and sterile regions. Colectomies are performed in more than 90% of cases in patients with widespread and severe resistant colitis. As one might assume based on the fact that most severe exacerbations develop during early stages diseases, about 2/3 of colectomies are performed in the first 2 years after diagnosis. The presence of widespread colitis at diagnosis was an independent predictor of colectomy over 10 years in the IBSEN study. The risk of colectomy in patients with widespread colitis is 4 times higher than in patients with ulcerative proctitis. However, the same study showed that patients with proximal colonic inflammation had a higher risk of colectomy than those with widespread colitis at diagnosis. In general, patients are younger (<30 лет), больные с распространенным колитом, скоростью оседания эритроцитов >30 mm/h and the presence of indications for corticosteroid therapy at the time of diagnosis are 15 times more likely to undergo colectomy.
The presence of systemic symptoms, such as weight loss and fever secondary to widespread colitis, further increases the risk of colectomy. At the same time, these factors do not affect the risk of exacerbation, which indicates that a severe attack of the disease fundamentally affects the outcome of the disease. A small proportion of patients with widespread colitis and systemic manifestations who managed to avoid colectomy during timely drug therapy had fewer exacerbations than patients without systemic symptoms (data from the IBSEN study and the Copenhagen cohort study). Epidemiologically identified patterns were also confirmed by endoscopic research: healing of the mucous membrane 1 year after the start of treatment in patients with widespread colitis with systemic symptoms predicted a good response to drug therapy.
Colorectal cancer
Inflammation of the colon mucosa and its damage active forms oxygen can lead to genetic changes and malignant growth. According to an analysis of the Belgian national registry, CRC in patients with UC in 73% develops in the area affected by colitis. Non-selective observation in the general population of patients indicates that the cumulative incidence of CRC development is 0 .4 and 1.1% for 10 and 20 years, respectively. The overall risk of CRC in patients was comparable to the background risk of CRC in the general population, as shown by meta-regression analysis in the same study. The cumulative incidence of CRC in other studies was higher and reached 10-20% after 10-20 years from the onset of the disease, but mainly increased in patients with total colitis observed in specialized centers.A higher incidence of CRC was observed in patients with a longer duration of the disease, concomitant PSC and in those in whom the disease began in At the same time, in a Belgian study, greater age at diagnosis was identified as an independent risk factor for CRC, which developed quite early, up to 8 years from diagnosis. Advanced colitis, male gender, and young age at diagnosis were also factors associated with increased mortality in UC patients with CRC. The incidence of CRC in patients with UC has decreased in recent decades and in 1999-2008. was only 1/3 of that in 1979-1988, probably due to the successful use of biological drugs and immunosuppressants. The IBSEN study also confirmed existing evidence that CRC does not significantly increase mortality in UC compared with the general population. Currently, the prognosis for patients with UC is the same as in the general population: 5-year survival is about 50%. According to a meta-analysis that included 1932 patients with UC, taking 5-aminosalicylic acid (5-ASA) helps reduce the risk of colorectal cancer. The role of 5-ASA in the chemoprevention of CRC in UC, given the decreasing incidence of cancer, may not be as great as previously thought. In patients with UC with concomitant PSC, when the risk of CRC is significantly increased, taking ursodeoxycholic acid, which reduces the level of secondary bile acids, which are carcinogens that increase the risk of CRC, especially in the right parts of the colon, can be considered promising. However, 2010 guidelines recommended against the use of ursodeoxycholic acid as chemoprophylaxis for CRC, based on results from a prospective follow-up study showing that patients taking high doses of ursodeoxycholic acid had an increased incidence of dysplasia and CRC.
Screening for colorectal cancer in patients with UC is recommended to be carried out 8-10 years after the onset of total colitis and after 15 years in patients with left-sided colitis. Patients with ulcerative proctitis do not require additional monitoring. Periodicity further observation determined by risk factors. A study based on the Belgian national registry showed that the time to development of colorectal cancer was independently influenced by: age at the onset of IBD and duration of IBD. Greater age at diagnosis of IBD predisposed to more rapid development of CRC. A significant number of cases of colorectal cancer detection simultaneously with the first confirmation of ulcerative colitis in this study indicates the need for a more cautious approach to monitoring older patients. In patients with UC and PSC, the risk of CRC is increased by 3 times compared to individuals suffering from UC only. In this group of patients, the cumulative incidence of colorectal cancer was 33 and 40%, respectively, 20 and 30 years after diagnosis. In patients with UC with concomitant PSC, screening colonoscopy is recommended annually from the time of diagnosis. Patients newly diagnosed with PSC should undergo colonoscopy to identify possible concomitant UC. In addition, the risk increases 2-3 times in patients with UC who have close relatives who suffered from colorectal cancer. If a relative develops cancer before the age of 50, the risk of a patient with UC increases by 9 times. Chromoendoscopy has been shown to be superior to traditional colonoscopy with biopsies of random mucosal sites in identifying areas of dysplasia. Confocal laser endomicroscopy increases the frequency of detection of dysplasia foci by 2.5 times compared with chromoendoscopy and by 4.75 times compared with traditional colonoscopy with random biopsy.
The mortality rate of patients with UC is not increased compared to the general population. A slight increase in mortality is found in patients over 60 years of age with underlying medical conditions who undergo emergency colectomy.
Treatment of ulcerative colitis
Modern therapy of mild and moderate ulcerative colitis
Once the severity has been assessed and excluded infectious nature diseases, therapy for mild and moderate UC is determined by the extent of the lesion, which is determined by colonoscopy. The goal of treatment is to control active inflammation and maintain the achieved remission. Treatment of active disease is usually a combination of topical and/or oral medications 5-ASA and corticosteroids. IN long term Maintenance therapy aims to reduce the duration of corticosteroid use due to its side effects (eg, infections and osteoporosis) and includes long-term use of 5-ASA, often with the addition of azathioprine. Regardless of drug choice, disease control is critical to reducing the overall risk of CRC in patients with a long history of the disease by reducing prolonged severe inflammation.
Mild to moderate active proctitis
The basis for the induction and maintenance of remission in mild and moderate UC is the use of 5-ASA drugs, which apparently act through the activation of nuclear receptors that affect inflammation, cell proliferation, apoptosis and metabolism of colon epithelial cells. With active proctitis, treatment is directed directly to the rectum: in this situation, suppositories with mesalazine, according to a meta-analysis that compared two dosage forms (oral and local), were more effective than taking the drug orally, and allowed to achieve remission after 2 weeks. This drug is usually prescribed at a dose of 500 mg 2 times a day or 1 g/day and is considered to be safe, easily tolerated and effective in patients with active proctitis and distal colitis. The choice of local therapy depends on the extent of the lesion. The suppositories act for 10-15 cm, the foam reaches 15-20 cm, and the enema allows you to deliver the medicine to the left bend. Disadvantages of treatment include bloating and leakage of medication, which can lead to non-compliance with the treatment regimen. Local corticosteroids are also used to accelerate the induction of remission, but they are ineffective in maintaining it. At the same time, in left-sided colitis, topical steroids demonstrate efficacy comparable to systemic corticosteroids, with less suppression of cortisol levels. A complete response often cannot be achieved with local therapy alone. In this case, oral mesalazine is added to treatment, which has been shown to achieve faster and more complete relief. intestinal symptoms than when using oral-only or rectal-only medications.
Mild to moderate distal active colitis
As with the lack of effectiveness of treatment for active proctitis, combination therapy increases the likelihood of achieving remission to a greater extent than monotherapy. The combination of enemas and oral mesalazine resulted in remission in 64% of patients compared with 43% receiving oral mesalazine and placebo enemas in a randomized, double-blind trial. At the same time, a dose-dependent effect is observed for oral therapy with 5-ASA. The ASCEND III study (a study to confirm comparable effectiveness) showed that of 389 patients receiving mesalazine extended release, when taking 4.8 g / day, treatment was effective in 70%, while when taking 2.4 g / day day the effect was observed in 66%. However, significantly more patients achieved clinical remission at weeks 3 and 6 of therapy when receiving 4.8 g rather than 2.4 g. In the ASCEND I study, comparing 4.8 and 2.4 g of the drug with a delayed release of mesalazine, statistically significant differences were found in the subgroup of patients with moderate active colitis: the effectiveness of treatment was 72 and 57%, respectively. Considering the relationship between side effects and therapeutic response, in patients with moderate form diseases, it is preferable to prescribe high doses of the drug.
In general, 5-ASA preparations are affordable and easily tolerated. However, some patients experience varying degrees of nausea, vomiting, dyspepsia, and anorexia, which reduces compliance. More severe reactions include pancreatitis, hepatotoxicity, bone marrow suppression, interstitial nephritis and anemia. In addition, 5-ASA, namely sulfasala-1ine, can have an effect on the structure of spermatozoa, which disappears after the end of administration. In 1-2% of patients, 5-ASA therapy can worsen the course of UC and should be discontinued.
Mild to moderate widespread colitis
Patients with active inflammation extending beyond the distal colon should initially be treated with oral 5-ASA. It has been shown that taking 4.8 g of mesalazine per day reduces the time to normalization of stool frequency and the disappearance of blood impurities compared with a dose of 2.4 g. A decrease in symptoms by the 2nd week was observed in 73 and 61% of patients, respectively. In addition, symptomatic relief by day 14 of therapy predicts continued remission an additional 2 weeks later, making day 14 the point at which intensification of therapy should be considered. Oral prednisolone should be added to treatment if symptoms are not relieved by oral 5-ASA alone. Based on an acceptable ratio between the therapeutic effect and possible side effects, a dose of 20 to 60 mg is traditionally recommended. Relative risk of developing opportunistic infections with long-term use corticosteroid levels are higher in patients over 50 years of age, so steroids are used with caution in them. Although randomized trials various schemes steroid dose reductions have not been carried out; usually, after symptoms have subsided, a slow dose reduction of 5 mg per week to 15-20 mg/day is recommended.
Inclusion of budesonide (Cortiment) in treatment regimens
Budesonide, which has minimal corticosteroid activity due to extensive first-pass hepatic metabolism, is now available as an alternative to prednisolone. Budesonide (Cortiment) is a sustained-release enteric-coated tablet that dissolves in the terminal ileum and is approved for the treatment of mild to moderate advanced UC. In a randomized comparison of the drug at a dose of 6 and 9 mg with mesalazine and placebo, the remission rate at week 8 was 17.9, 13.2 and 12.1%, respectively, with a placebo efficacy of 7.4%. Budesonide 9 mg was more effective than placebo in achieving clinical remission in patients with active mild to moderate UC. Since this drug does have side effects of traditional corticosteroids, the duration of its use should ideally be limited to 8 weeks.
Maintaining remission
Further therapy for remission of UC is determined by the extent of the lesion. Azathioprine or mercaptopurine may be used to overcome hormonal dependence or in patients with an insufficient response to aminosalicylates monotherapy. When compared within a randomized clinical trial 2 mg/kg azathioprine and 3.2 g mesalazine in hormone-dependent UC patients achieved clinical remission in 53% versus 21%, respectively. Side effects include depression of bone marrow function (primary leukopenia), abnormal liver function tests, and intolerance reactions such as fever, rash, myalgia, or arthralgia. Before prescribing these drugs, thiopurine methyltransferase genotype analysis should be performed as this allows dose selection and identification of patients at risk for possible drug toxicity. Long-term severe inflammation is a proven risk factor for neoplasia. The importance of mucosal healing should be emphasized, as this outcome of treatment not only reduces the risk of cancer, but also, as shown in a prospective study, reduces the risk of colectomy and further use of steroids.
Modern therapy of moderate and severe ulcerative colitis
Symptoms of UC result from inflammation of the large intestine, which consists of the colon and rectum. Most symptoms of UC are caused by inflammation of the rectum. The severity of your symptoms and some additional information can help you determine which therapy is right for you. For example, patients with 4 or more bowel movements per day or other manifestations such as fever or anemia are classified as having moderate to severe active colitis. Your current symptoms allow you to determine exactly the severity of the disease.
Your treatment will include a remission induction period, during which we will try to suppress inflammatory activity so you get better, and a second remission maintenance period, which aims to maintain your health and prevent future flare-ups. As a chronic disease, UC requires ongoing treatment in order to fully control the disease and avoid the low but possible risk of colorectal cancer.
For moderate UC, the most commonly used class of drugs is aminosalicylates. Aminosalicylates are a group of non-immune suppressive drugs that act locally on the intestinal wall to reduce inflammation. These drugs presented in various forms, are capable of inducing and maintaining remission of this form of UC and can be prescribed in combination with other treatments for more severe UC. To increase effectiveness, they are prescribed both orally and rectally. These drugs are extremely safe, but 3% of people may experience intolerance and even worsening diarrhea after starting to take them. There is also a very small risk of kidney failure, which periodic blood tests to assess kidney function can help rule out.
Most patients with moderate to severe UC require corticosteroids. Steroids are extremely effective and quick remedy induction of remission, used mainly because of the speed of response to treatment. They are generally safe when taken short-term, but we try our best to reduce the duration of their use due to the danger of side effects with long-term use and quickly reduce the dose. Topical steroids in the form of a foam or enema may be used to treat the rectum and lower colon. The most common side effects of short-term steroid therapy are sleep disturbances, weight gain, anxiety, acne, and mood changes. Steroids are not suitable for maintaining remission. A new type of steroid, budesonide (Cortiment*), acts primarily locally in the colon and has fewer side effects than prednisolone, so may be useful in treating less severe forms of the disease.
In some patients with UC, another group of drugs that suppress the immune system, thiopurines, may also be effective. These drugs, which include azathioprine (Imuran® or Azasan) and mercaptopurine (Purinegol), are prescribed to help you stop taking steroids and avoid them in the future. Thiopurines are taken orally once a day. Their mechanism of action is not fully understood, although we know that they suppress the growth of white blood cells, which play a key role in the development of inflammation. Common but preventable side effects include a decrease in the number of white cells in the blood, which recovers when the drug is stopped and should be monitored with periodic blood tests. Some side effects depend on how a particular patient's body processes the medicine. Fortunately, understanding how this happens can be done with a simple blood test before treatment begins. Rarer effects include infections and a small increase in the incidence of non-melanomatous skin cancer and lymphoma. This risk can be reduced by getting vaccinated against flu and pneumonia, limiting exposure to sunlight, and getting an annual checkup with a dermatologist. The risk of lymphoma is extremely small, but slightly increased compared to the general population. It increases with the duration of taking the drug and with the age of the patient, but is eliminated when therapy is stopped.
Another type of treatment is biological therapy, the use of anti-TNF drugs. They are antibodies to TNF, a mediator of inflammation. Because these are protein drugs, they must be administered intravenously or subcutaneously. There are currently three anti-TNF drugs approved for the treatment of UC in the United States, including infliximab (Remicade), adalimumab (Humira), and golimumab (Simponi). This therapy is extremely effective for this form of UC and becomes even more effective when combined with thiopurines. Side effects include a slightly increased risk of infections and rarely allergic reactions to treatment, which may also indicate a loss of response. To protect patients from these reactions, we screen patients for tuberculosis and hepatitis B and vaccinate them against influenza and pneumonia before starting treatment.
A recent addition to our arsenal is vedolizumab (Entyvio), which is also an intravenous biologic but works by inhibiting the migration of white blood cells from the bloodstream into the intestine. Because of this specific mechanism of action, the use of vedolizumab represents a more targeted and fairly safe approach to the treatment of UC, although it does not significantly increase the risk of nasopharyngeal infections. Vedolizumab can be used for both induction and maintenance of remission.
In some cases, severe UC may require hospitalization, during which intravenous therapy is administered to achieve remission. A small proportion of patients have to undergo surgical treatment. Surgery for severe UC involves removing the entire colon and rectum. With the removal of the colon, a person is cured of UC. In most patients, it is possible to form a “new” rectum from the small intestine - a J-shaped reservoir.
Moderate active UC is characterized by the presence of four or more bowel movements per day with minimal overall impact of the disease on the body, while with severe UC, frequent, more than 6 times a day, bloody stools are combined with general changes in the body (fever, tachycardia, anemia or increase in erythrocyte sedimentation rate).
The main goal of therapy is to induce remission, after which treatment is selected to prevent further use of steroids. In general, the choice of maintenance therapy is determined by which drug was required to induce remission. A more stringent criterion for effective therapy, which is increasingly used, is endoscopic remission (healing of the mucosa), the presence of which reduces the need for corticosteroids, the frequency of hospitalization, the risk of colectomy and cancer, and also increases the chances of sustained clinical remission.
When treating mild to moderate active UC, it is initially preferred to prescribe aminosalicylates due to the convenience of selecting their dose and high safety. Sulfasalazine at a daily dose of 4-6 g is an effective and inexpensive means of inducing and maintaining remission, but more often leads to side effects. Mesalazine, olsalazine and balsalazide have the same proven effectiveness in inducing and maintaining remission in moderate-severe UC. Their effect is further enhanced by prescribing a dose of 4.8 g/day and simultaneous administration of the drug locally into the rectum in the form of suppositories or enemas. Intolerance to mesalazine is rare, in contrast to sulfasalazine, for which it is very common.
Many patients with moderately active UC and patients with severe UC must be prescribed treatments that affect the immune system. In patients with aminosalicylate failure or hormonal dependence, thiopurines may be effective, but their slow onset of action makes them unsuitable for inducing remission and therefore usually requires concomitant administration of steroids or anti-TNF agents. The use of thiopurines in UC does not have a high-quality evidence base; Thus, it is unclear whether they should be prescribed together with aminosalicylates or as monotherapy.
Under the action of the enzyme thiopurine methyltransferase, thiopurines are converted into 6-thioguanine and 6-methylmercaptopurine. The latter may cause an increase in liver enzyme levels. Achieving remission is due to the action of 6-thioguanine, but this same metabolite leads to suppression of bone marrow function in patients with low thiopurine methyltransferase activity in the presence of high levels of 6-thioguanine. In patients with normal thiopurine methyltransferase activity, the dose is selected based on body weight at the rate of 2-3 mg/kg azathioprine and 1-1.5 mg/kg mercaptopurine.
Currently a quality indicator medical care is to assess the activity of thiopurine methyltransferase before starting treatment with thiopurines. Lack of enzyme activity (0.3% of the population) is a contraindication to therapy. Patients with intermediate disease activity (11%) should initially receive a low dose of the drug (25-50 mg) and increase it gradually (25-50 mg/week), while patients with normal enzyme activity can begin treatment immediately with the full dose . Bone marrow function and changes in liver enzyme levels should be monitored. We also recommend periodic analysis of thiopurine metabolite levels to optimize therapy, although these studies are not included in the standards of care. Increases in liver enzymes and bone marrow depression are dose-related side effects, while for intolerance reactions such as fever, rash, arthralgia and myalgia, a different thiopurine is usually sufficient. There is still a 50% chance of cross-reaction. A common side effect of this class of drugs is pancreatitis, which requires permanent discontinuation of thiopurine therapy. In addition, taking thiopurines increases the risk of non-melanoma skin cancer, infections, including serious ones, and lymphoma.
Anti-TNF therapy is an effective treatment option for patients with moderate to severe active UC, patients with hormone-dependent and hormone-resistant disease, and patients with ineffectiveness or intolerance to aminosalicylates or thiopurines. Infliximab, adalimumab and golimumab are approved for use in the United States to induce and maintain remission of UC. The likelihood of inducing and maintaining remission, as well as healing of the mucous membrane, increases with the simultaneous use of anti-TNF drugs and thiopurines. Combination therapy also helps to reduce immunogenicity (the formation of antibodies to the drug) and increase the residual level of anti-TNF drug in the blood. Such data were obtained using infliximab/adalimumab in combination with azathioprine for UC, but recent studies suggest the advisability of prescribing methotrexate, which should be preferred in patients with an increased risk of lymphoma (men <30 and >50 years). Data on combination therapy with golimumab are still accumulating.
Secondary loss of response to anti-TNF therapy has been well studied. If it occurs, infections and the possibility of accelerated elimination of the drug due to the formation of antibodies to it should be excluded. For infliximab and adalimumab, kits are available on the market to determine their serum levels and drug antibodies. In patients who have previously responded to anti-TNF therapy but then develop antibodies to the drug and the drug itself is not detectable in the serum, it is reasonable to prescribe a different anti-TNF drug. Recently, treatment tactics have been changing: we are trying to control not only the symptoms of the disease, but also endoscopic activity in order to prevent exacerbations and the development of colonic dysplasia, but a clear scheme for such monitoring has not yet been developed. At the same time, the use of fecal calprotectin for non-invasive monitoring disease activity.
Vedolizumab, an α 4 β 7 integrin inhibitor, is effective in inducing and maintaining remission in moderate to severe active UC, regardless of whether the patient has previously received anti-TNF drugs. Available data indicate its high safety, low immunogenicity and high sustained response rates.
Patients with fulminant UC or patients with severe UC and intolerance/failure to induce remission with maximum doses of oral steroids, oral and topical aminosalicylates, and anti-TNF agents require hospitalization and intravenous hormonal therapy. If remission is not achieved after 3 days of intravenous steroid treatment, there is an increased likelihood that further use will not be effective. In such a situation, the possibility of appointing complementary therapy infliximab or calcineurin inhibitors.
Salvage therapy to induce remission with calcineurin inhibitors (tacrolimus or cyclosporine) avoids colectomy in 82% of patients with severe hormone-resistant colitis. After achieving remission, patients continue maintenance therapy with thiopurines or anti-TNF drugs. When switching from one immunosuppressant to another, careful monitoring of possible infectious complications is required. We recently described the use of calcineuron inhibitors to induce remission followed by maintenance therapy with vedolizumab. Within 10 years from the diagnosis of UC, colectomy is performed in a total of 10-17% of patients, and among patients hospitalized for severe UC, urgent colectomy is necessary in 27% of cases. The “gold standard” of surgery is multi-stage surgical treatment with the formation of an ileoanal pouch anastomosis (IAPA) using a hardware or manual method.
